Get the free New Patient/Medical History Form
Show details
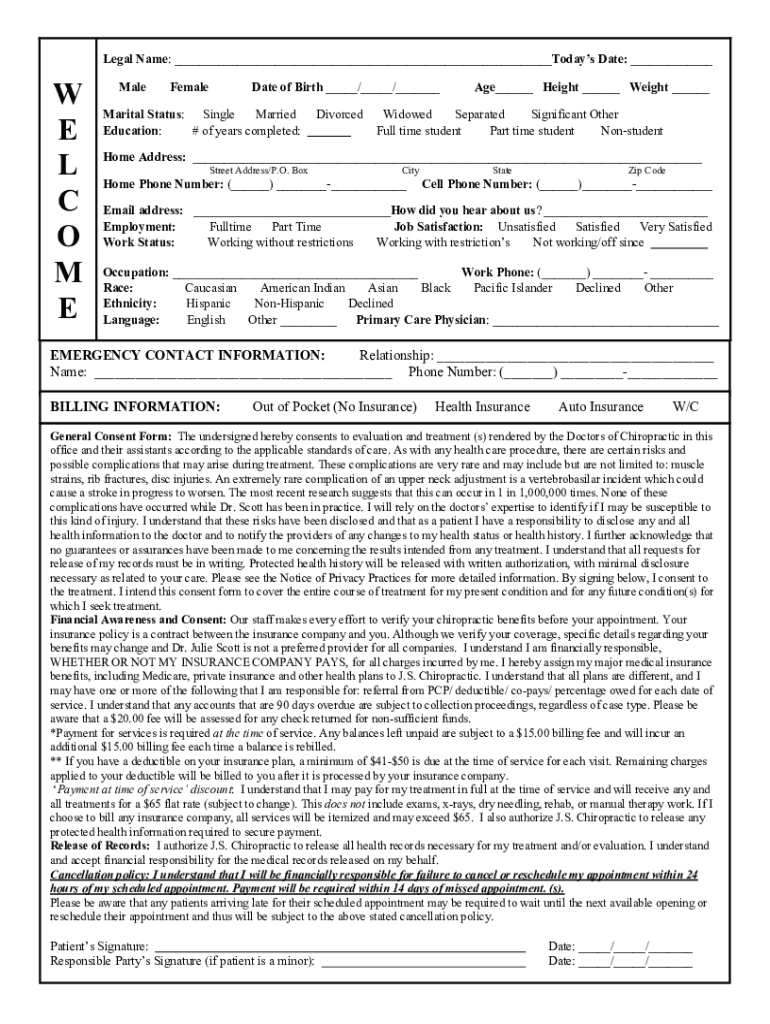
Legal Name: ___Today's Date: ___W
E
L
C
O
M
EMaleFemaleDate of Birth ___/___/___Marital Status: Single
Married
Education:
# of years completed:Divorced___ Height ___ Weight ___Widowed
Separated
Significant
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign new patientmedical history form
Edit your new patientmedical history form form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your new patientmedical history form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit new patientmedical history form online



Here are the steps you need to follow to get started with our professional PDF editor:
1
Log in to your account. Click on Start Free Trial and register a profile if you don't have one yet.
2
Upload a file. Select Add New on your Dashboard and upload a file from your device or import it from the cloud, online, or internal mail. Then click Edit.
3
Edit new patientmedical history form. Add and change text, add new objects, move pages, add watermarks and page numbers, and more. Then click Done when you're done editing and go to the Documents tab to merge or split the file. If you want to lock or unlock the file, click the lock or unlock button.
4
Get your file. When you find your file in the docs list, click on its name and choose how you want to save it. To get the PDF, you can save it, send an email with it, or move it to the cloud.
pdfFiller makes dealing with documents a breeze. Create an account to find out!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out new patientmedical history form
How to fill out new patientmedical history form
01
Start by providing personal information such as name, date of birth, address, and contact information.
02
Fill out any pertinent medical history, including previous surgeries, chronic conditions, and allergies.
03
List current medications being taken, including dosage and frequency.
04
Provide information about any family history of medical conditions.
05
Detail any lifestyle factors such as smoking, alcohol consumption, and exercise habits.
06
Sign and date the form to confirm accuracy and consent.
Who needs new patientmedical history form?
01
New patients visiting a healthcare provider for the first time will need to fill out a new patient medical history form.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I send new patientmedical history form for eSignature?
Once your new patientmedical history form is complete, you can securely share it with recipients and gather eSignatures with pdfFiller in just a few clicks. You may transmit a PDF by email, text message, fax, USPS mail, or online notarization directly from your account. Make an account right now and give it a go.
How do I fill out new patientmedical history form using my mobile device?
Use the pdfFiller mobile app to fill out and sign new patientmedical history form. Visit our website (https://edit-pdf-ios-android.pdffiller.com/) to learn more about our mobile applications, their features, and how to get started.
How do I edit new patientmedical history form on an Android device?
You can edit, sign, and distribute new patientmedical history form on your mobile device from anywhere using the pdfFiller mobile app for Android; all you need is an internet connection. Download the app and begin streamlining your document workflow from anywhere.
What is new patient medical history form?
New patient medical history form is a document used to gather information about a patient's past and current medical conditions, treatments, and other relevant health details.
Who is required to file new patient medical history form?
New patients visiting a healthcare facility or provider are required to file a new patient medical history form.
How to fill out new patient medical history form?
To fill out a new patient medical history form, patients need to provide accurate information about their medical history, medications, allergies, surgeries, and any other relevant health details as accurately as possible.
What is the purpose of new patient medical history form?
The purpose of new patient medical history form is to provide healthcare providers with essential information to deliver proper care and treatment to the patient.
What information must be reported on new patient medical history form?
Information such as past medical conditions, current medications, allergies, surgical history, family medical history, and contact information must be reported on new patient medical history form.
Fill out your new patientmedical history form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
New Patientmedical History Form is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms





If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
