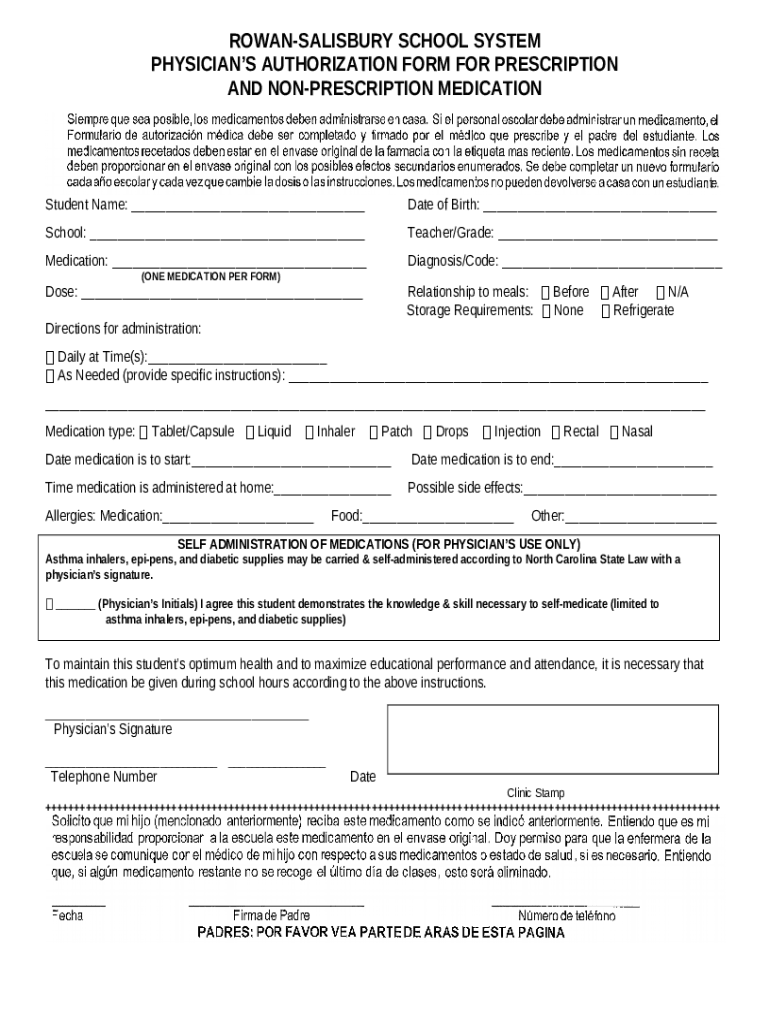



What is PHYSICIAN'S AUTHORIZATION FOR ... Form?
The PHYSICIAN'S AUTHORIZATION FOR ... is a fillable form in MS Word extension that should be submitted to the relevant address to provide some information. It must be filled-out and signed, which can be done manually in hard copy, or by using a certain software e. g. PDFfiller. It allows to fill out any PDF or Word document right in the web, customize it according to your purposes and put a legally-binding electronic signature. Right after completion, you can send the PHYSICIAN'S AUTHORIZATION FOR ... to the appropriate receiver, or multiple recipients via email or fax. The blank is printable as well thanks to PDFfiller feature and options presented for printing out adjustment. Both in digital and physical appearance, your form will have a clean and professional appearance. You can also turn it into a template for later, without creating a new document again. All you need to do is to amend the ready form.
Template PHYSICIAN'S AUTHORIZATION FOR ... instructions
Once you are ready to start submitting the PHYSICIAN'S AUTHORIZATION FOR ... word template, you have to make certain that all required information is well prepared. This part is highly important, as far as mistakes may lead to unwanted consequences. It is distressing and time-consuming to re-submit forcedly entire editable template, letting alone the penalties caused by missed deadlines. To work with your digits takes a lot of concentration. At first glance, there is nothing challenging in this task. Nonetheless, it's easy to make an error. Experts suggest to record all sensitive data and get it separately in a different document. When you've got a sample so far, it will be easy to export it from the file. Anyway, it's up to you how far can you go to provide true and legit information. Doublecheck the information in your PHYSICIAN'S AUTHORIZATION FOR ... form carefully when completing all required fields. You can use the editing tool in order to correct all mistakes if there remains any.
PHYSICIAN'S AUTHORIZATION FOR ...: frequently asked questions
1. I need to fill out the document with very sensitive data. Shall I use online solutions to do that, or it's not that safe?
Services dealing with sensitive information (even intel one) like PDFfiller are obliged to give safety measures to customers. We offer you::
- Cloud storage where all data is kept protected with encryption. The user is the only who has got to access their personal files. Doorways to steal this information is strictly prohibited all the way.
- To prevent forgery, every single file obtains its unique ID number upon signing.
- Users are able to use some extra security features. They are able to set authentication for receivers, for example, request a photo or password. In PDFfiller you can store .doc forms in folders protected with layered encryption.
2. Have never heard about e-signatures. Are they the same comparing to physical ones?
Yes, it is absolutely legal. After ESIGN Act concluded in 2000, an electronic signature is considered like physical one is. You can fill out a word file and sign it, and it will be as legally binding as its physical equivalent. While submitting PHYSICIAN'S AUTHORIZATION FOR ... form, you have a right to approve it with a digital solution. Be certain that it matches to all legal requirements as PDFfiller does.
3. I have a spread sheet with some of required information all set. Can I use it with this form somehow?
In PDFfiller, there is a feature called Fill in Bulk. It helps to export data from document to the online template. The key benefit of this feature is that you can use it with Excel sheets.