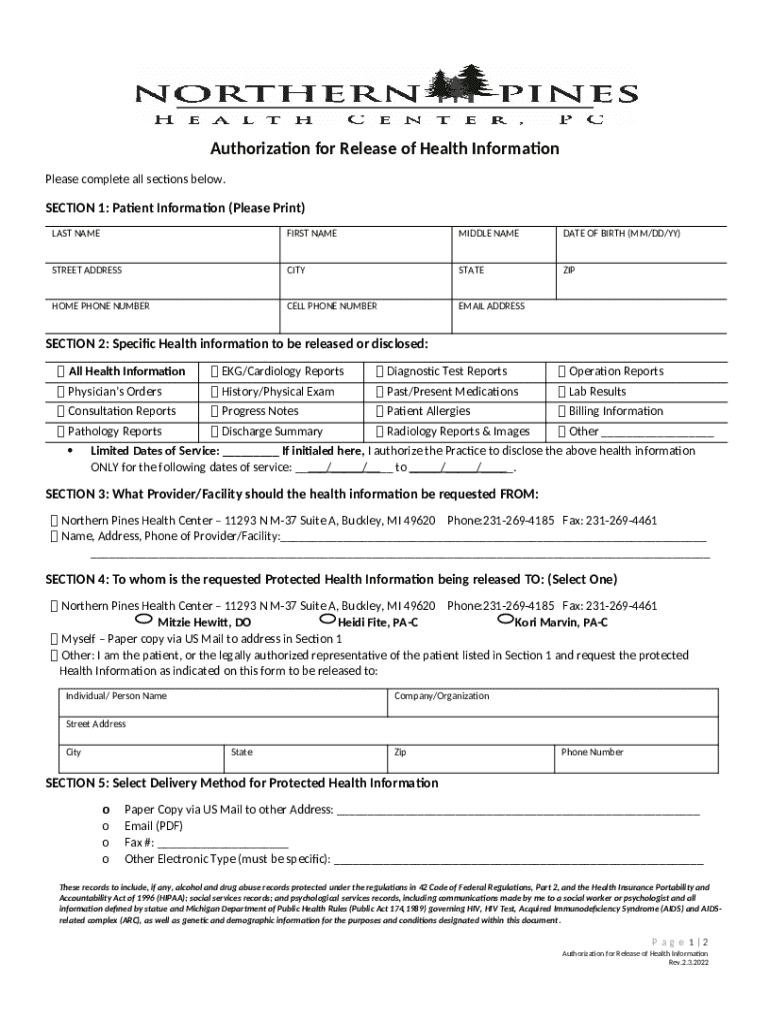







What is SECTION 1: Patient Ination (Please Print) Form?
The SECTION 1: Patient Ination (Please Print) is a fillable form in MS Word extension that should be submitted to the specific address to provide specific info. It must be completed and signed, which is possible manually in hard copy, or by using a particular solution e. g. PDFfiller. This tool allows to fill out any PDF or Word document directly in your browser, customize it according to your requirements and put a legally-binding electronic signature. Right after completion, user can easily send the SECTION 1: Patient Ination (Please Print) to the appropriate individual, or multiple ones via email or fax. The editable template is printable too due to PDFfiller feature and options offered for printing out adjustment. Both in electronic and physical appearance, your form should have a organized and professional appearance. Also you can turn it into a template to use it later, without creating a new file from the beginning. You need just to amend the ready form.
Template SECTION 1: Patient Ination (Please Print) instructions
Once you're about filling out SECTION 1: Patient Ination (Please Print) Word template, be sure that you have prepared enough of necessary information. That's a mandatory part, as far as some errors can cause unpleasant consequences from re-submission of the full word form and completing with missing deadlines and you might be charged a penalty fee. You ought to be observative enough when working with digits. At first sight, it might seem to be uncomplicated. Nonetheless, you can easily make a mistake. Some people use such lifehack as saving their records in another file or a record book and then attach it into document's template. However, come up with all efforts and provide actual and solid information in SECTION 1: Patient Ination (Please Print) word form, and doublecheck it when filling out all required fields. If you find any mistakes later, you can easily make amends when working with PDFfiller tool without blowing deadlines.
How to fill out SECTION 1: Patient Ination (Please Print)
In order to start filling out the form SECTION 1: Patient Ination (Please Print), you'll need a template of it. If you use PDFfiller for filling out and submitting, you can obtain it in several ways:
- Look for the SECTION 1: Patient Ination (Please Print) form in PDFfiller’s library.
- You can also upload the template from your device in Word or PDF format.
- Create the writable document to meet your specific purposes in PDFfiller’s creator tool adding all necessary fields via editor.
Regardless of what choice you prefer, you will have all features you need for your use. The difference is that the template from the catalogue contains the necessary fillable fields, and in the rest two options, you will have to add them yourself. However, this procedure is dead simple and makes your sample really convenient to fill out. The fields can be easily placed on the pages, as well as removed. Their types depend on their functions, whether you’re entering text, date, or put checkmarks. There is also a e-signature field if you need the word file to be signed by others. You can sign it yourself with the help of the signing tool. Once you're done, all you have to do is press the Done button and pass to the form submission.