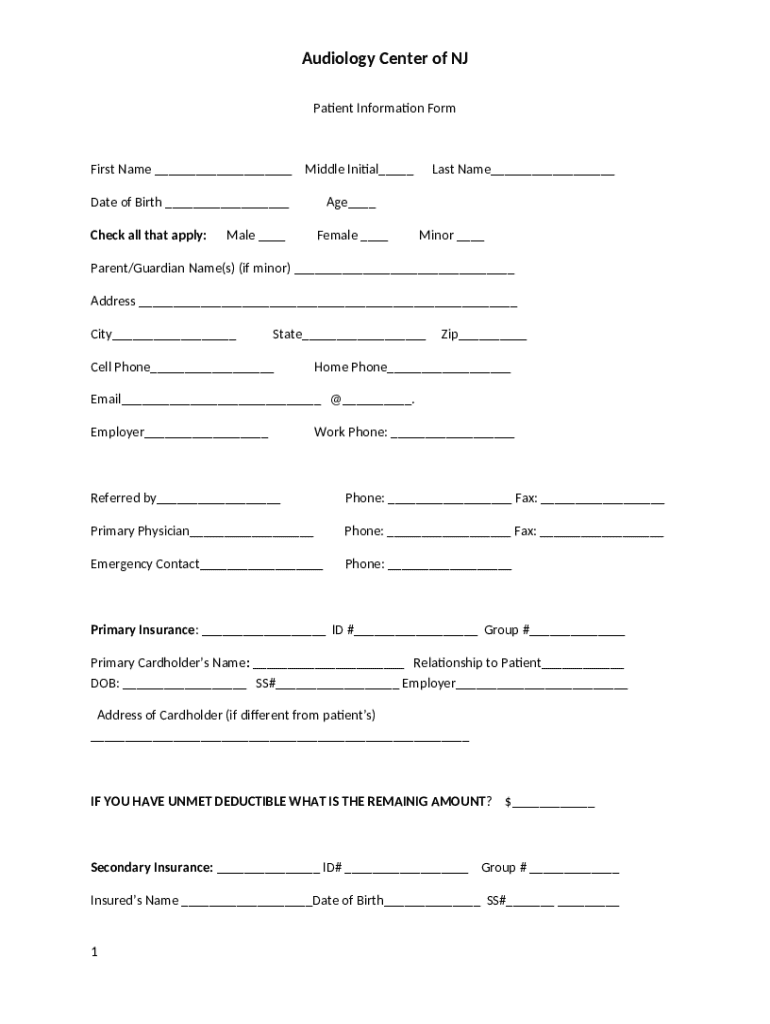







What is Patient Ination Form?
The Patient Ination is a fillable form in MS Word extension that can be filled-out and signed for certain purpose. Then, it is provided to the relevant addressee to provide specific info and data. The completion and signing is available in hard copy or via a trusted application like PDFfiller. These tools help to complete any PDF or Word file without printing them out. While doing that, you can edit it according to the needs you have and put a legal electronic signature. Once you're good, the user ought to send the Patient Ination to the recipient or several ones by mail and also fax. PDFfiller offers a feature and options that make your Word form printable. It has a variety of settings for printing out. It does no matter how you'll deliver a form - in hard copy or by email - it will always look professional and clear. To not to create a new editable template from the beginning all the time, make the original file into a template. Later, you will have a customizable sample.
Instructions for the form Patient Ination
Prior to start completing the Patient Ination form, you need to make clear that all the required information is prepared. This very part is highly significant, as long as mistakes may result in undesired consequences. It is really uncomfortable and time-consuming to resubmit the whole word form, not to mention penalties resulted from missed due dates. Working with figures takes more concentration. At first glance, there’s nothing challenging in this task. Nonetheless, there's nothing to make an error. Experts advise to store all required information and get it separately in a different document. When you have a sample, you can just export that data from the file. In any case, it's up to you how far can you go to provide true and legit info. Check the information in your Patient Ination form twice when filling all necessary fields. You are free to use the editing tool in order to correct all mistakes if there remains any.
How to fill out Patient Ination
First thing you need to start to fill out the form Patient Ination is writable template of it. If you complete and file it with the help of PDFfiller, look at the ways listed below how you can get it:
- Search for the Patient Ination form in the PDFfiller’s library.
- If you have the very form in Word or PDF format on your device, upload it to the editing tool.
- If there is no the form you need in filebase or your storage space, create it by yourself with the editing and form building features.
Regardless of the variant you prefer, you are able to edit the document and put different fancy elements in it. Except for, if you want a form that contains all fillable fields out of the box, you can obtain it in the catalogue only. Other options are short of this feature, so you'll need to place fields yourself. Nonetheless, it is quite easy and fast to do. When you finish this, you will have a useful sample to be submitted. The fillable fields are easy to put when you need them in the document and can be deleted in one click. Each function of the fields corresponds to a separate type: for text, for date, for checkmarks. If you want other individuals to put signatures in it, there is a corresponding field too. E-signature tool enables you to put your own autograph. Once everything is completely ready, hit the Done button. After that, you can share your form.