
Get the free Provider Appeal Request Form
Show details
This form is used by healthcare providers to appeal the denial of claims or authorizations by Preferred Care Network, requiring the submission of supporting documentation.
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign provider appeal request form
Edit your provider appeal request form form online
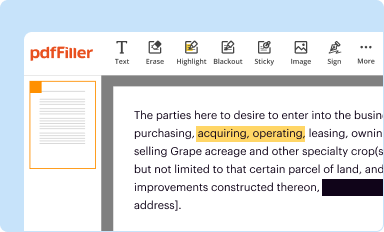
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
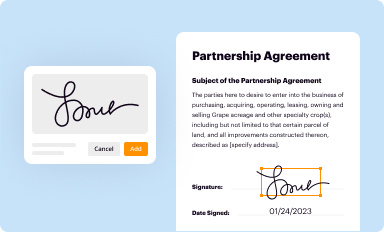
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
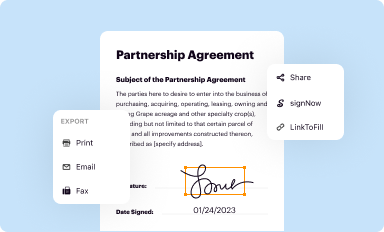
Share your form instantly
Email, fax, or share your provider appeal request form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit provider appeal request form online



In order to make advantage of the professional PDF editor, follow these steps below:
1
Set up an account. If you are a new user, click Start Free Trial and establish a profile.
2
Prepare a file. Use the Add New button to start a new project. Then, using your device, upload your file to the system by importing it from internal mail, the cloud, or adding its URL.
3
Edit provider appeal request form. Text may be added and replaced, new objects can be included, pages can be rearranged, watermarks and page numbers can be added, and so on. When you're done editing, click Done and then go to the Documents tab to combine, divide, lock, or unlock the file.
4
Save your file. Select it from your list of records. Then, move your cursor to the right toolbar and choose one of the exporting options. You can save it in multiple formats, download it as a PDF, send it by email, or store it in the cloud, among other things.
With pdfFiller, it's always easy to deal with documents. Try it right now
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out provider appeal request form
How to fill out provider appeal request form
01
Obtain the provider appeal request form from your insurance company's website or customer service.
02
Read the instructions carefully before starting to fill out the form.
03
Enter the provider's name, address, and contact information in the designated sections.
04
Provide the patient's information, including their name, policy number, and contact details.
05
Clearly state the reason for the appeal, including relevant details and any supporting documentation.
06
Include dates of service and any relevant claim numbers associated with the appeal.
07
Review the form for accuracy and completeness before submitting.
08
Sign and date the form where required.
09
Submit the completed form to the appropriate address as indicated in the instructions.
Who needs provider appeal request form?
01
Healthcare providers who have had a claim denied or require a reconsideration of a decision made by an insurance company.
02
Patients seeking to have their claims reviewed or appealed by their healthcare provider.
Comprehensive Guide to the Provider Appeal Request Form
Understanding the Provider Appeal Request Form
The provider appeal request form is a formal document used by healthcare providers to appeal decisions made by insurance companies regarding claims and reimbursements. This form is critical in the healthcare ecosystem as it provides a structured method for providers to challenge denials, seeking resolution and ensuring that patients receive appropriate care without financial barriers.
The importance of this form lies in its ability to streamline communication between healthcare providers and insurers. By utilizing a standardized format, it increases the likelihood of a timely review and decision on an appeal. Typical scenarios requiring this form include denied claims for medical services, authorization requests for services not initially approved, or adjustments to previously accepted claims based on new information.
Key features of pdfFiller’s Provider Appeal Request Form
pdfFiller offers a robust provider appeal request form that is easy to use and designed to meet the needs of today’s healthcare professionals. This cloud-based solution allows users to access the form from anywhere, making it ideal for busy medical practices and teams working remotely.
Accessibility from anywhere: Whether in the office or at home, healthcare providers can complete the form anytime, aiding timely appeals.
Seamless editing and signing capabilities: Users can easily fill out, edit, and sign the form digitally without the hassle of printing and scanning.
Collaboration tools: Teams can collaboratively work on the provider appeal request form, with options for real-time editing and feedback.
Step-by-step instructions for filling out the Provider Appeal Request Form
Filling out the provider appeal request form can seem daunting, but following these steps will simplify the process. Preparation is key — start by gathering all necessary information, including patient details, provider information, and relevant documentation that supports the appeal.
Collect required documents such as insurance policy information, patient identification, prior claim details, and denial letters.
Access the Provider Appeal Request Form through pdfFiller, using the direct links provided.
Fill out the form: Complete each section, providing patient information, provider details, and clearly stating the reason for the appeal.
Edit the form using pdfFiller’s tools to ensure accuracy, concentrating on completeness and clarity.
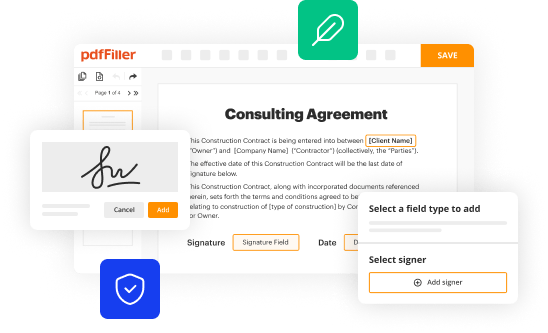
Sign the form electronically. Utilize pdfFiller’s eSignature options to obtain all necessary signatures before submitting.
Interactive tools available on pdfFiller
pdfFiller enhances the user experience with a variety of interactive tools designed for efficient form management. The platform integrates with cloud storage solutions like Google Drive and Dropbox, providing users with streamlined access to their documents.
Key features include document tracking, which allows users to monitor the progress of submitted appeals, and versatile templates that save time in future submissions. This level of organization helps providers focus on patient care, rather than paperwork.
Collaborating on appeals with teams
Collaboration is crucial when working on appeals, and pdfFiller facilitates this through its shared access feature. Teams can easily share the provider appeal request form for review, enabling colleagues to provide feedback and suggestions in real-time.
With features that allow for commenting and collaborative editing, multiple team members can contribute to the preparation of the form. This synergy not only speeds up the appeal process but also improves the overall quality of submissions thanks to diverse insights from different professionals.
Frequently asked questions (FAQs) about the Provider Appeal Request Form
Several common questions arise when dealing with the provider appeal request form. One frequent concern is what to do if an appeal is denied. In such cases, providers should carefully review the denial reasons and gather any additional evidence or documentation that may support a second appeal submission.
What to do if your appeal is denied? Review denial reasons and consider submitting more documentation or a clear explanation.
Time limits for submitting appeals: Be aware of the specific timeline set by the insurance provider, typically ranging from 30 to 120 days.
Additional tips for successful submissions: Always double-check for errors and ensure that the form is fully completed before submission.
Legal considerations and best practices
Understanding the legal implications surrounding appeals and documentation is vital for healthcare providers. Maintaining compliance with regulations like HIPAA is essential when handling patient information during the appeals process. Mistakes in documentation can lead to legal issues or further claim denials.
Best practices include keeping thorough records of all communications related to appeals, ensuring that every submission is supported by adequate documentation, and directly communicating with insurers when questions arise. This diligence will facilitate smoother resolutions of appeals.
Helpful links and resources
To assist users in navigating the appeals process, a collection of resources is available. Various healthcare appeals resources provide detailed guidelines on submitting appeals, including governmental websites and professional organizations dedicated to healthcare compliance.
Links to relevant healthcare appeals resources, including CMS guidelines.
Templates and forms available on pdfFiller for comprehensive document management.
Contact information for support regarding the form and appeals process if further assistance is required.
Signup for email updates
Receiving updates about form changes and best practices can be highly beneficial for users of the provider appeal request form. Subscribing to pdfFiller's email newsletters ensures that you are always informed about any modifications and tips that may enhance your experience.
For those interested, subscribing is a straightforward process, often involving a simple sign-up form on the pdfFiller website. Keeping abreast of updates guarantees that you are maximizing the tool’s potential in managing appeals.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How do I fill out the provider appeal request form form on my smartphone?
You can easily create and fill out legal forms with the help of the pdfFiller mobile app. Complete and sign provider appeal request form and other documents on your mobile device using the application. Visit pdfFiller’s webpage to learn more about the functionalities of the PDF editor.
How can I fill out provider appeal request form on an iOS device?
pdfFiller has an iOS app that lets you fill out documents on your phone. A subscription to the service means you can make an account or log in to one you already have. As soon as the registration process is done, upload your provider appeal request form. You can now use pdfFiller's more advanced features, like adding fillable fields and eSigning documents, as well as accessing them from any device, no matter where you are in the world.
How do I complete provider appeal request form on an Android device?
Complete your provider appeal request form and other papers on your Android device by using the pdfFiller mobile app. The program includes all of the necessary document management tools, such as editing content, eSigning, annotating, sharing files, and so on. You will be able to view your papers at any time as long as you have an internet connection.
What is provider appeal request form?
The provider appeal request form is a document used by healthcare providers to appeal a decision made by a payer regarding claims, reimbursements, or coverage related to medical services.
Who is required to file provider appeal request form?
Healthcare providers, such as physicians, hospitals, and clinics, that wish to contest a decision made by an insurance company or government payers must file a provider appeal request form.
How to fill out provider appeal request form?
To fill out the provider appeal request form, providers should enter their contact information, details about the patient and services rendered, the specific decision being appealed, and attach any relevant documentation supporting their case.
What is the purpose of provider appeal request form?
The purpose of the provider appeal request form is to formally challenge decisions made by payers regarding claims, allowing providers to seek reconsideration and potentially secure rightful payment for services rendered.
What information must be reported on provider appeal request form?
The provider appeal request form must report information including the provider's details, patient information, claim number, date of service, reason for appeal, and any supporting documentation or evidence.
Fill out your provider appeal request form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Provider Appeal Request Form is not the form you're looking for?Search for another form here.
Relevant keywords
If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
