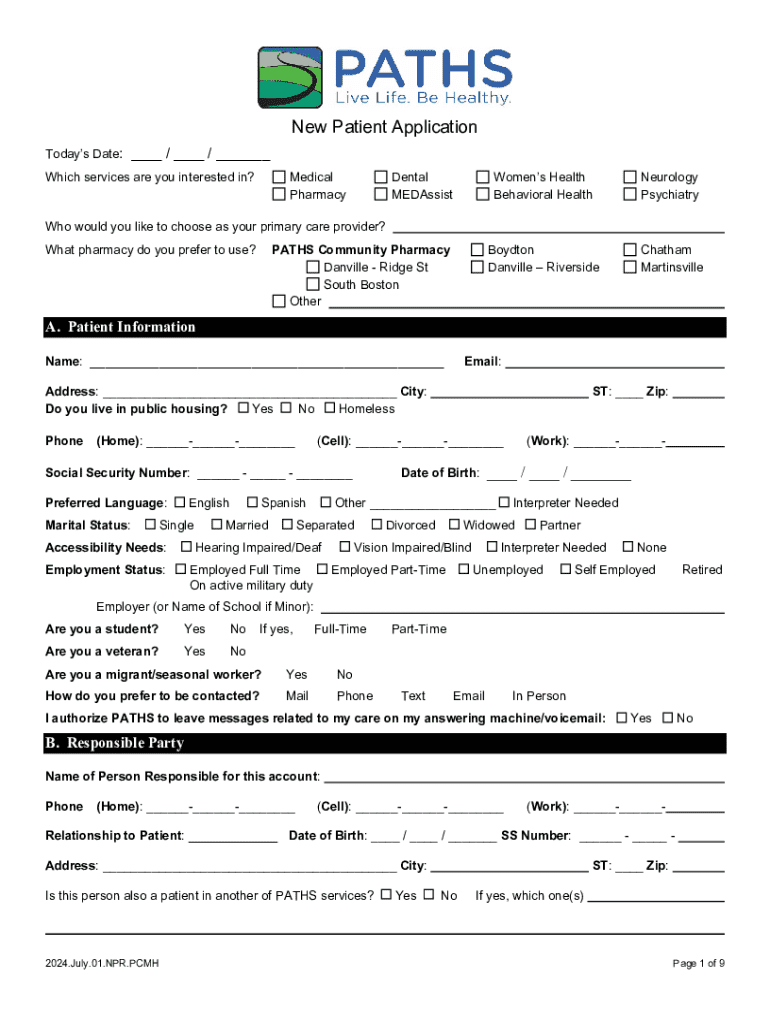
Get the free New Patient Application
Show details
Este documento es un formulario de solicitud para nuevos pacientes que buscan atención médica, dental y de salud comportamental, y contiene información sobre los servicios ofrecidos, preguntas
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign new patient application
Edit your new patient application form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your new patient application form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing new patient application online



To use the professional PDF editor, follow these steps:
1
Create an account. Begin by choosing Start Free Trial and, if you are a new user, establish a profile.
2
Prepare a file. Use the Add New button. Then upload your file to the system from your device, importing it from internal mail, the cloud, or by adding its URL.
3
Edit new patient application. Rearrange and rotate pages, add and edit text, and use additional tools. To save changes and return to your Dashboard, click Done. The Documents tab allows you to merge, divide, lock, or unlock files.
4
Get your file. When you find your file in the docs list, click on its name and choose how you want to save it. To get the PDF, you can save it, send an email with it, or move it to the cloud.
Dealing with documents is always simple with pdfFiller.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out new patient application
How to fill out new patient application
01
Start by collecting basic personal information: Full name, date of birth, and contact details.
02
Provide insurance information: Include the name of your insurance provider, policy number, and group number.
03
Fill out medical history: List any past illnesses, surgeries, allergies, and current medications.
04
Include emergency contact information: Name and phone number of someone to contact in case of an emergency.
05
Sign and date the application form to confirm that the information provided is accurate and complete.
06
Submit the application form to the healthcare provider's office, either in person or via their online portal if available.
Who needs new patient application?
01
Anyone seeking to establish care with a new healthcare provider needs to fill out a new patient application.
02
Individuals who have recently moved to a new area and require a local physician must complete the application.
03
Patients changing their healthcare provider for any reason, such as dissatisfaction with their current provider, also need to fill out a new patient application.
04
Newly insured individuals who are choosing a new healthcare provider as part of their insurance plan requirements.
Your Comprehensive Guide to the New Patient Application Form
Understanding the new patient application form
The new patient application form is an essential document used in healthcare to gather important information from individuals seeking to receive medical services. This form serves not only as an introduction between the patient and healthcare provider but also as a vital means of collecting necessary data to ensure proper care. By filling out this application, patients provide health professionals with critical details regarding their history, insurance information, and current health status, which aid in tailored treatment plans.
The importance of the new patient application form cannot be overstated. In a fast-paced healthcare environment, having complete and accurate information from the outset can significantly impact the quality of care. A well-completed form can assist in quick diagnosis and treatment, while incomplete or incorrect information can lead to delays and complications in care.
Key components of the new patient application form
A comprehensive new patient application form typically includes several key components that ensure all relevant information is collected. These sections drive the efficiency and effectiveness of patient care.
This includes vital details such as full name, address, and contact information, along with date of birth and Social Security number for identification purposes.
Patients need to provide information about their primary and secondary insurance providers, including policy numbers, to ensure coverage and payment processes are streamlined.
A summary of previous medical conditions, surgeries, current medications, and allergies is essential for informing future treatments.
Patients should list an emergency contact, along with any special instructions in case of unforeseen events during visits.
Preparation steps for filling out the form
Before sitting down to fill out the new patient application form, it's crucial to gather the necessary documents. Having all pertinent information at your fingertips will streamline the process, ensuring accuracy and completeness.
Make sure to have your state-issued ID or driver's license and your health insurance cards readily available.
If you have records from past providers or relevant referral letters, collect these to provide comprehensive medical history.
Reviewing the form layout before filling it out can save time and prevent confusion. Most forms contain suggested sections indicating what information is required. Additionally, identify any areas where you have questions or need clarification.
Step-by-step instructions for completion
Completing the new patient application form requires careful attention to detail. Following these steps ensures a comprehensive and accurate submission.
When entering personal details, ensure names match your identification and check for typos that could lead to complications. Avoid leaving sections blank; instead, mark them as 'N/A' if not applicable.
To verify your insurance coverage, check your provider’s website or call customer service. Accurately jot down policy numbers to avoid claim issues.
Summarize key medical records succinctly to give a complete picture of your health. Honesty in disclosing previous treatments and conditions is critical.
Choose someone trustworthy and accessible. Ensure they are aware they are listed and can provide necessary assistance if needed.
Editing and reviewing the new patient application form
After completing the new patient application form, take the time to edit and review it for any errors or missing information. pdfFiller offers various editing tools that make this process effortless. You can easily make changes to any section and verify that you have provided all necessary details.
It’s also recommended to utilize interactive features within pdfFiller that help identify any missing fields or check for common errors. This not only ensures accuracy but aids in a smoother submission process.
Digital signature and submission process
Once your application form is complete and reviewed, the next step is to add your digital signature. Using pdfFiller’s eSign capabilities makes signing simple and effective. After signing, review the guidelines to ensure that the digital signature adheres to legal standards.
Most healthcare providers accept digitally signed forms submitted via their patient portal, email, or through dedicated healthcare apps.
If required to submit a hard copy, print the completed form ensuring all sections are legible, and send it using a secure postal method.
Managing your new patient application form
After submission, safeguarding your completed new patient application form is vital. With pdfFiller, you can store your document securely in the cloud, ensuring easy access anytime you need it.
As your health status changes or you change insurers, easily update your application in pdfFiller and follow the same submission process.
With pdfFiller, you can reuse information from previous forms which saves time on future visits and ensures continuity of care.
Benefits of using pdfFiller for your new patient application form
pdfFiller empowers users with a seamless platform for editing, signing, and managing their new patient application forms from anywhere. Rather than physical paperwork, the cloud-based system allows users to maintain easy access to their documents and to collaborate with healthcare providers effortlessly.
Editing tools allow you to make adjustments quickly, ensuring your form reflects current and accurate information.
Access your forms anytime, anywhere, which is especially useful for busy patients with tight schedules.
pdfFiller offers stringent security measures to protect sensitive patient information, ensuring peace of mind.
Common FAQs about new patient application forms
As you navigate the new patient application process, various questions might arise. Understanding common concerns can enhance your experience.
If you experience difficulties, refer to the help section of pdfFiller or contact customer support for assistance.
Processing times can vary, but your provider should provide an estimate. Following up directly can expedite any delays.
Always reach out to your chosen healthcare provider. They can guide you through the submission process and answer specific inquiries.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I edit new patient application on a smartphone?
You may do so effortlessly with pdfFiller's iOS and Android apps, which are available in the Apple Store and Google Play Store, respectively. You may also obtain the program from our website: https://edit-pdf-ios-android.pdffiller.com/. Open the application, sign in, and begin editing new patient application right away.
How do I fill out the new patient application form on my smartphone?
On your mobile device, use the pdfFiller mobile app to complete and sign new patient application. Visit our website (https://edit-pdf-ios-android.pdffiller.com/) to discover more about our mobile applications, the features you'll have access to, and how to get started.
How do I edit new patient application on an iOS device?
No, you can't. With the pdfFiller app for iOS, you can edit, share, and sign new patient application right away. At the Apple Store, you can buy and install it in a matter of seconds. The app is free, but you will need to set up an account if you want to buy a subscription or start a free trial.
What is new patient application?
A new patient application is a form that new patients fill out to provide necessary information to a healthcare provider before receiving care.
Who is required to file new patient application?
Any individual seeking to become a patient at a healthcare facility or practice is typically required to file a new patient application.
How to fill out new patient application?
To fill out a new patient application, one should provide personal details such as name, contact information, insurance details, medical history, and any other required information as specified by the healthcare provider.
What is the purpose of new patient application?
The purpose of the new patient application is to gather essential information about the patient to ensure proper care, create a patient record, and verify insurance coverage.
What information must be reported on new patient application?
The information that must be reported typically includes personal identification details, contact information, insurance information, medical history, allergies, and current medications.
Fill out your new patient application online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
New Patient Application is not the form you're looking for?Search for another form here.
Relevant keywords
If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
