Get the free Patient Request /authorization to Use and/or Disclose Protected Health Information
Show details
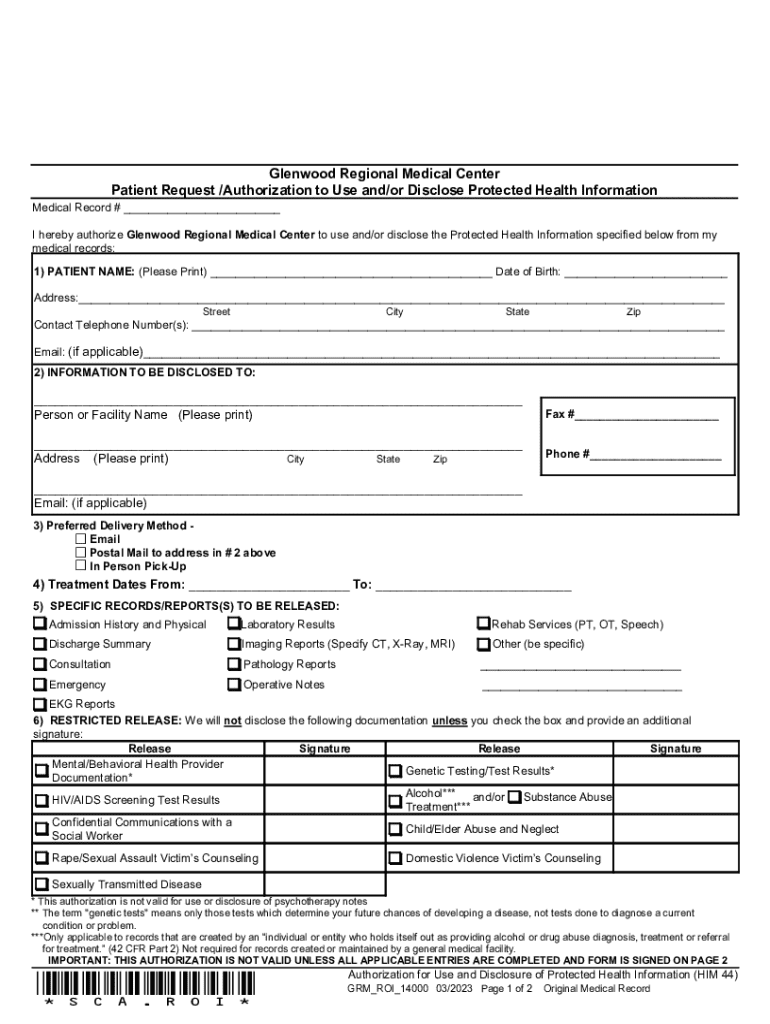
This document is an authorization form for patients to grant the Glenwood Regional Medical Center permission to use and disclose their protected health information for specified purposes.
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign patient request authorization to

Edit your patient request authorization to form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.

Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.

Share your form instantly
Email, fax, or share your patient request authorization to form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing patient request authorization to online



Follow the steps down below to take advantage of the professional PDF editor:
1
Log in to your account. Click Start Free Trial and sign up a profile if you don't have one yet.
2
Upload a document. Select Add New on your Dashboard and transfer a file into the system in one of the following ways: by uploading it from your device or importing from the cloud, web, or internal mail. Then, click Start editing.
3
Edit patient request authorization to. Add and replace text, insert new objects, rearrange pages, add watermarks and page numbers, and more. Click Done when you are finished editing and go to the Documents tab to merge, split, lock or unlock the file.
4
Get your file. Select the name of your file in the docs list and choose your preferred exporting method. You can download it as a PDF, save it in another format, send it by email, or transfer it to the cloud.
Dealing with documents is always simple with pdfFiller.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out patient request authorization to

How to fill out patient request authorization to
01
Gather all necessary patient information including name, date of birth, and medical record number.
02
Identify the healthcare provider or facility to which the authorization is being sent.
03
Clearly specify the type of information that is being requested (e.g., medical records, treatment history).
04
Include the time frame for which the information is being requested (e.g., specific dates of treatment).
05
Obtain the patient's signature and date on the authorization form to confirm permission.
06
Ensure that the form complies with all privacy regulations and laws.
07
Submit the completed authorization form to the designated provider or facility.
Who needs patient request authorization to?
01
Patients seeking access to their own medical records.
02
Healthcare providers requesting patient information from other providers.
03
Insurance companies needing patient information for claims processing.
04
Legal representatives representing the patient in medical matters.
Your Guide to Patient Request Authorization to Form
Understanding patient request authorization
Patient Request Authorization refers to the formal process where a patient grants permission for their healthcare provider to share specific medical information with designated individuals or organizations. This authorization is crucial in healthcare communication, ensuring that patients have control over who accesses their sensitive health information.
The importance of this authorization lies in the protection of patient privacy and the understanding that consent must be informed and voluntary. Typical use cases include sharing medical records with insurance companies, caregivers, or another healthcare provider for continuity of care or specific procedures.
Overview of the patient request authorization form
The Patient Request Authorization Form serves the vital purpose of documenting the patient’s consent to release medical information. This form acts as a safeguard for both the patient and the healthcare provider, ensuring that all parties are aware of the terms under which information is shared.
Includes the patient's full name, date of birth, and contact information.
Specifies the individual or organization authorized to receive the information.
Outlines the type of information to be shared, such as medical records or treatment plans.
Confirms the patient’s consent and records the date of authorization.
Preparing to fill out the form
Before filling out the Patient Request Authorization Form, it's essential to gather all necessary information. This includes identification documents, healthcare provider details, and specifics about the information that needs to be shared. Being organized ensures a smoother process and reduces the chance of errors.
Understanding healthcare regulations such as the Health Insurance Portability and Accountability Act (HIPAA) is critical since these laws protect your privacy. Additionally, be attentive to common mistakes; incomplete sections or unauthorized signatures can result in denial of the request.
Step-by-step instructions for completing the form
Completing the Patient Request Authorization Form can be straightforward if followed step-by-step.
Ensure to include your full name, date of birth, and any identifiers that your healthcare provider might require.
Clearly specify who you are authorizing. This could be a family member, a caregiver, or a third-party organization. Make sure they are aware.
Be specific about what information you are allowing to be shared. Indicate whether it pertains to medical history, treatment plans, or billing information.
Your signature validates the request. Ensure that it’s the correct person signing. Wherever digital options are available, consider using pdfFiller for an electronic signature.
Interactive tools to enhance your experience
Using pdfFiller for your Patient Request Authorization Form can greatly enhance your experience. The platform's robust PDF editing capabilities allow you to fill out forms quickly and accurately. This eliminates the frustration of having to print, complete, and scan documents back into electronic format.
Moreover, with the eSign options available, you can sign documents electronically, ensuring a seamless experience. Additionally, pdfFiller facilitates collaboration; if you're part of a healthcare team, you can share and edit forms with team members for a collective approach to managing patient information.
Managing your patient request authorization form
Once you've completed your Patient Request Authorization Form, it's important to manage it properly. Store completed forms in an organized manner, ensuring that you have access to them when needed. Using pdfFiller allows you to access your forms from anywhere since it’s a cloud-based solution.
It's also wise to keep a copy for your records, especially when dealing with insurance claims. This can help streamline communication with your healthcare provider and insurance company.
Troubleshooting common issues
Despite careful preparation, issues can arise during the process. If you encounter problems with form submission—such as online portals not accepting your form—check for common errors like missing fields or incorrect formatting.
If your request is denied, contact the healthcare provider directly for clarification. They can provide insights into why the authorization was not accepted and what can be done to rectify the situation.
Frequently asked questions (FAQs)
Typically, the healthcare provider will process your request and send the requested information to the designated recipient within a certain timeframe.
Processing times can vary but healthcare regulations often require a response within 30 days.
Yes, you can revoke your authorization request, but it's important to communicate this in writing to the healthcare provider.
Best practices for authenticated requests
To ensure your Patient Request Authorization is honored, follow best practices such as providing complete and accurate information. Double-check every field for completeness and explore whether additional documents or identification might help support your request.
In addition, maintain the security and privacy of your information. Use secure methods for sharing your authorization and be aware of what types of data you are consenting to share.
Why choose pdfFiller for patient request authorization forms
Choosing pdfFiller for your Patient Request Authorization Form offers unique benefits that streamline your document management process. With features designed specifically for healthcare documentation, pdfFiller allows you to edit PDFs, eSign, and collaborate seamlessly from one platform.
Users often share testimonials about pdfFiller's efficiency and ease of use, highlighting how it has made their experiences with document management far more manageable. This cloud-based solution not only saves time but also reduces the stress associated with paperwork.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How do I edit patient request authorization to in Chrome?
Install the pdfFiller Chrome Extension to modify, fill out, and eSign your patient request authorization to, which you can access right from a Google search page. Fillable documents without leaving Chrome on any internet-connected device.
Can I sign the patient request authorization to electronically in Chrome?
Yes. You can use pdfFiller to sign documents and use all of the features of the PDF editor in one place if you add this solution to Chrome. In order to use the extension, you can draw or write an electronic signature. You can also upload a picture of your handwritten signature. There is no need to worry about how long it takes to sign your patient request authorization to.
How do I edit patient request authorization to on an iOS device?
Create, modify, and share patient request authorization to using the pdfFiller iOS app. Easy to install from the Apple Store. You may sign up for a free trial and then purchase a membership.
What is patient request authorization to?
Patient request authorization is a formal process where a patient gives consent for their healthcare provider to share specific medical information with other parties, such as insurance companies or other healthcare providers.
Who is required to file patient request authorization to?
Typically, the healthcare provider or their administrative staff is required to file patient request authorization on behalf of the patient, ensuring that proper consent is obtained before sharing medical information.
How to fill out patient request authorization to?
To fill out patient request authorization, the patient must provide their personal information, specify the information that can be shared, identify the recipients of the information, indicate the purpose of sharing, and sign and date the form.
What is the purpose of patient request authorization to?
The purpose of patient request authorization is to protect patient privacy while allowing for necessary sharing of medical information among healthcare providers and entities involved in patient care or billing.
What information must be reported on patient request authorization to?
Patient request authorization must include the patient's full name, date of birth, details of the information to be shared, names of the recipients, purpose for sharing, duration of authorization, and the patient's signature.
Fill out your patient request authorization to online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Patient Request Authorization To is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms




If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
