Get the free PATIENT HISTORY FORM Name
Show details
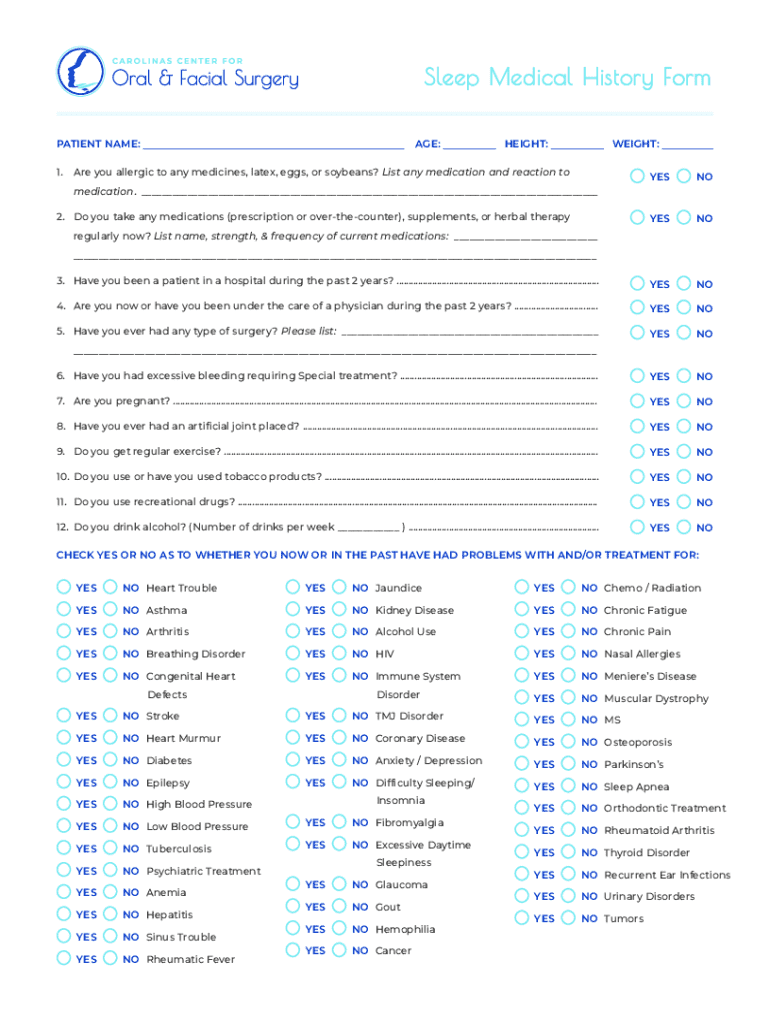
Sleep Medical History Form PATIENT NAME: 1.AGE:HEIGHT:WEIGHT:Are you allergic to any medicines, latex, eggs, or soybeans? List any medication and reaction toYESNOYESNO3. Have you been a patient in
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign patient history form name
Edit your patient history form name form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your patient history form name form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing patient history form name online



Follow the guidelines below to benefit from the PDF editor's expertise:
1
Log in. Click Start Free Trial and create a profile if necessary.
2
Simply add a document. Select Add New from your Dashboard and import a file into the system by uploading it from your device or importing it via the cloud, online, or internal mail. Then click Begin editing.
3
Edit patient history form name. Add and replace text, insert new objects, rearrange pages, add watermarks and page numbers, and more. Click Done when you are finished editing and go to the Documents tab to merge, split, lock or unlock the file.
4
Save your file. Choose it from the list of records. Then, shift the pointer to the right toolbar and select one of the several exporting methods: save it in multiple formats, download it as a PDF, email it, or save it to the cloud.
Dealing with documents is always simple with pdfFiller.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out patient history form name
How to fill out patient history form name
01
Start with personal information: Enter the patient's full name, date of birth, and contact details.
02
Provide medical history: Include any previous illnesses, surgeries, or chronic conditions.
03
List medications: Note any current medications, dosages, and frequency.
04
Note allergies: Specify any known allergies to medications, food, or other substances.
05
Family history: Include relevant health conditions that run in the family.
06
Review lifestyle: Mention details about smoking, alcohol use, diet, and exercise habits.
07
Complete additional sections: Fill out any other sections as instructed, such as insurance information or emergency contacts.
Who needs patient history form name?
01
New patients at a healthcare facility.
02
Physicians or healthcare providers conducting a medical assessment.
03
Insurance companies for coverage evaluations.
04
Researchers or clinical studies requiring patient data.
05
Caregivers or family members managing patient health.
Patient History Form Name Form: A Comprehensive How-to Guide
Understanding the patient history form
A patient history form is a crucial document in healthcare that gathers comprehensive information about a patient’s medical background. It serves as a foundational tool for healthcare providers to understand the patient’s past and present health conditions, thus facilitating informed medical decisions. This form not only helps in diagnosing conditions accurately but also ensures that treatments are tailored appropriately.
The importance of the patient history form in medical settings cannot be overstated. For healthcare providers, it forms the basis for patient assessments, aiding in identifying risk factors and potential complications. For patients, it creates an opportunity to share vital information that may influence their healthcare outcomes.
Key components of the form
Personal Information: This includes the patient’s name, address, contact information, and date of birth.
Medical History: An overview of past illnesses, surgeries, and chronic conditions.
Current Medications: A list of all medications the patient is currently taking, including over-the-counter drugs and supplements.
Allergies and Reactions: Information about any known allergies and adverse reactions to medications.
Family Medical History: A summary of health conditions present in the patient's family, which can indicate hereditary risks.
How to access the patient history form
Accessing the patient history form is a straightforward process. Many healthcare facilities provide this form online through their websites, aiming to streamline patient check-ins for appointments.
Online availability
On pdfFiller, you can easily find the patient history form template. Simply navigate to the search bar and type 'patient history form name form' to locate the specific document. Once located, it’s as easy as clicking to start filling it out directly.
Downloading options
For those who prefer offline access, pdfFiller offers multiple download options. You can download the form as a PDF, which is ideal for printing. Additionally, if your workflows require it, you may also opt to download the form in Word or Excel formats. To download a PDF, simply click the ‘Download’ button once you've selected the form.
Filling out the patient history form
Filling out the patient history form correctly is vital for ensuring your healthcare provider has all necessary information. Here’s a step-by-step guide to assist you in this process.
Gather Necessary Information: Before beginning, ensure you have your medical records and information regarding your medications and allergies.
Filling Out Personal Information: Write your name, address, contact details, and other requested personal information clearly.
Documenting Medical History: Provide accurate accounts of past illnesses, treatments, and surgeries in detail.
Listing Current Medications: Ensure to list all medications, including dosages and frequencies.
Reporting Allergies and Family History: Be thorough in this section, as it could significantly influence treatment options.
Tips for accurate completion
For an error-free experience, accuracy is paramount. Always double-check the information before submitting. If unsure about a detail, consult with your healthcare provider to verify.
Common mistakes to avoid
Missing sections is a frequent issue that can lead to incomplete medical records. Also, be cautious of inaccuracies, especially regarding medical data and allergies, as these can lead to severe health implications.
Editing and customizing the patient history form
One of the powerful features of using pdfFiller is the ability to edit and customize your patient history form. This ensures that the document fits your specific needs, whether you're a patient or a healthcare provider.
Accessing the editing tools on pdfFiller
Upon selecting your form, you can use various editing tools provided by pdfFiller. This includes the ability to add text, checkmarks, and annotations. If certain sections of the form do not apply to you or your practice, you can even remove them for clarity.
Personalizing the form for specific needs
If you are a healthcare provider, consider modifying fields based on your practice's specific requirements. You might want to include additional sections pertinent to your specialty or add special instructions or notes concerning the patient's care.
Signing and submitting the patient history form
Once you have completed the patient history form, the next step is often signing and submitting it. This process has been simplified through digital tools, especially when using pdfFiller.
eSigning made easy
The electronic signature feature on pdfFiller allows for a quick and secure signing process. Navigate to the sign option, follow the prompts, and you can add a legally binding signature that can be stored securely with your form.
Submitting your completed form
After signing, you have several options for submission, such as emailing the completed document directly to your healthcare provider, printing it out, or sharing it online. Always consider keeping a personal copy for your records, which is vital in case of any future queries regarding your healthcare history.
Managing your patient history forms
Managing your patient history forms effectively can significantly reduce administrative burdens. With pdfFiller's document management features, keeping track of various forms and patient data becomes seamless.
Organizing your documents
Utilize folders and tags on pdfFiller to categorize your documents. You can organize forms by patient, treatment type, or date, ensuring easy retrieval whenever needed. Best practice includes maintaining a consistent naming convention, making it easier to locate documents across your system.
Collaboration features for teams
If you’re working as part of a healthcare team, pdfFiller’s collaboration features are invaluable. The platform allows you to share documents with colleagues effortlessly. Utilize commenting and review tools to enhance communication and ensure everyone is on the same page when it comes to patient care.
Frequently asked questions (FAQs)
What if I forget to include information? You can always edit the form later, but it's crucial to note that missing information can impact care.
How can I retrieve a previously filled form? Use the search function in your pdfFiller account to find and access past documents.
What are my options for form storage? pdfFiller provides secure cloud storage, ensuring your documents are safely backed up and easy to access.
Conclusion and next steps
Accurate patient history is vital for effective healthcare delivery. Taking the time to fill out the patient history form carefully can significantly impact diagnosis and treatment. By utilizing the robust features provided by pdfFiller, you can streamline the process of managing healthcare documents.
We encourage individuals and healthcare teams to engage with pdfFiller not only for the patient history form name form but also for a variety of other documents. The capability to edit, eSign, and manage documents from a single, cloud-based platform empowers users dramatically, making healthcare administration smoother and more efficient.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I get patient history form name?
It's simple using pdfFiller, an online document management tool. Use our huge online form collection (over 25M fillable forms) to quickly discover the patient history form name. Open it immediately and start altering it with sophisticated capabilities.
How do I execute patient history form name online?
pdfFiller has made it simple to fill out and eSign patient history form name. The application has capabilities that allow you to modify and rearrange PDF content, add fillable fields, and eSign the document. Begin a free trial to discover all of the features of pdfFiller, the best document editing solution.
Can I edit patient history form name on an Android device?
You can make any changes to PDF files, like patient history form name, with the help of the pdfFiller Android app. Edit, sign, and send documents right from your phone or tablet. You can use the app to make document management easier wherever you are.
What is patient history form name?
The patient history form is commonly referred to as the 'Patient Health History Form'.
Who is required to file patient history form name?
Patients are required to fill out the Patient Health History Form, along with healthcare providers or administrative staff who may assist.
How to fill out patient history form name?
To fill out the Patient Health History Form, patients should provide accurate and complete information about their medical history, including any past illnesses, surgeries, medications, allergies, and family medical history.
What is the purpose of patient history form name?
The purpose of the Patient Health History Form is to gather essential medical information that helps healthcare providers understand a patient's health background and make informed treatment decisions.
What information must be reported on patient history form name?
The information that must be reported on the Patient Health History Form includes personal details, previous medical conditions, surgical history, current medications, allergies, and family health history.
Fill out your patient history form name online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Patient History Form Name is not the form you're looking for?Search for another form here.
Relevant keywords
If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
