Last updated on Mar 26, 2026
Get the free COBRA Election Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
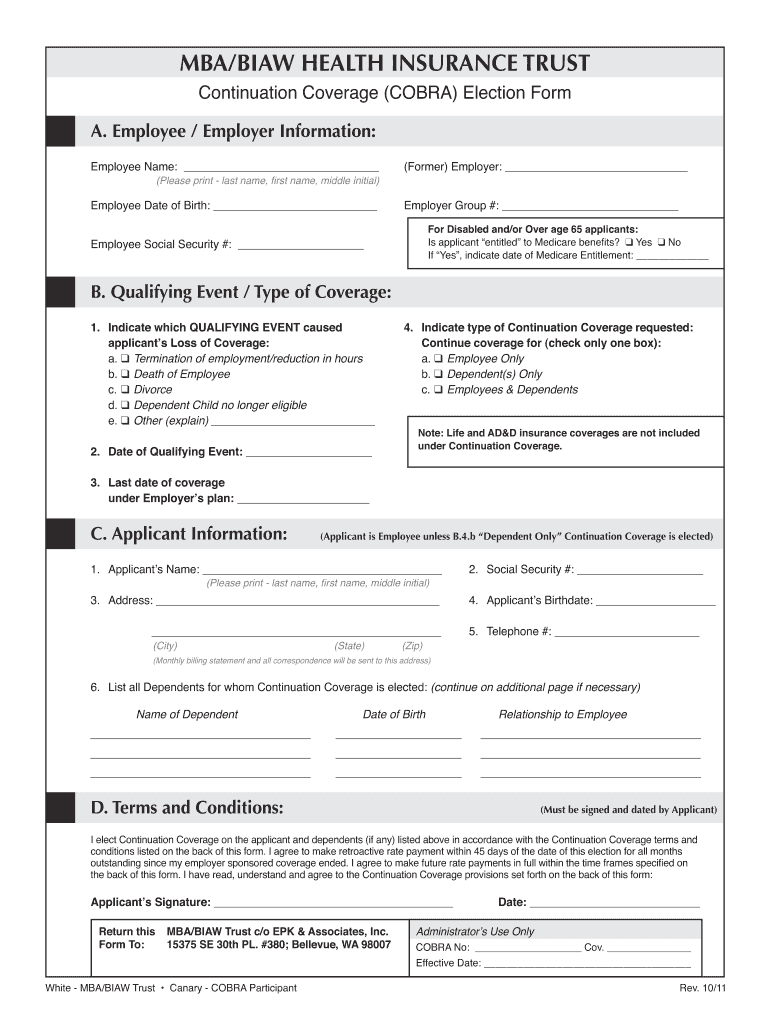
What is cobra election form
The COBRA Election Form is a healthcare document used by individuals who have experienced a qualifying event to elect continuation coverage under the Consolidated Omnibus Budget Reconciliation Act (COBRA).
pdfFiller scores top ratings on review platforms
Who needs cobra election form?
Explore how professionals across industries use pdfFiller.

Cobra election form is needed by:
-
Employees losing health insurance coverage after a job change
-
Dependents needing continued health insurance benefits
-
Employers managing COBRA compliance requirements
-
Human resources professionals assisting staff with benefits
-
Insurance brokers aiding clients with health coverage options
Comprehensive Guide to cobra election form
Understanding the COBRA Election Form
The COBRA Election Form is a crucial document that enables individuals to elect continuation coverage under the Consolidated Omnibus Budget Reconciliation Act (COBRA). This form serves to protect individuals who have experienced qualifying events, such as job loss, which would otherwise lead to the loss of health insurance coverage. Filling out this form helps ensure that applicants maintain essential health coverage during transitions in employment or personal circumstances.
Electing continuation coverage not only provides immediate health insurance security but also can significantly impact the financial stability of those recovering from unexpected life changes. Understanding the importance of the COBRA election form ensures that individuals are informed about their rights and options for maintaining necessary health care services.
Purpose and Benefits of Completing the COBRA Election Form
Completing the COBRA Election Form promptly and accurately comes with several benefits. Firstly, it allows individuals to preserve their health insurance coverage, preventing interruptions in medical care. This continuation coverage can be essential for managing existing health conditions, receiving routine preventive care, and avoiding high out-of-pocket costs associated with uninsured medical services.
Moreover, timely submission provides peace of mind, as individuals can focus on their recovery or job search without the added stress of losing health coverage. By filling out the form correctly, applicants can ensure they and their dependents remain protected, maintaining both health and financial security.
Who Needs the COBRA Election Form?
Various individuals may find themselves in situations requiring the COBRA Election Form. Common qualifying events that necessitate filing this form include:
-
Job loss
-
Reduction in hours
-
Divorce or legal separation
-
Death of the covered employee
-
Loss of dependent status (e.g., aging out of coverage)
Understanding the eligibility criteria is essential for both applicants and their dependents. Knowing who needs this form is a vital step towards ensuring sustained access to health care during challenging times.
How to Fill Out the COBRA Election Form Online
Filling out the COBRA Election Form online can streamline the process significantly. Here’s a step-by-step guide:
-
Access the COBRA Election Form through a reliable platform like pdfFiller.
-
Fill in your personal information, including your employee name.
-
Provide details regarding your qualifying event, such as the date you lost your job.
-
Include information about any dependents for whom you are electing continuation coverage.
-
Review the completed form for accuracy and completeness.
-
Sign and date the form before submitting it.
Utilizing an online platform like pdfFiller facilitates a smoother filling process and helps track changes efficiently, ensuring all information is recorded correctly.
Common Errors and How to Avoid Them
When completing the COBRA Election Form, applicants often make several common mistakes. These pitfalls can hinder the processing of your application:
-
Missing required signatures
-
Incorrect dates
-
Incomplete sections of the form
-
Providing incorrect information about dependents
To avoid these mistakes, take the time to carefully review the form before submission. Familiarize yourself with the instructions, and consider asking a knowledgeable friend or family member to proofread the completed document to ensure its accuracy.
Filing and Submission Guidelines for the COBRA Election Form
Submitting the COBRA Election Form accurately and within designated timeframes is crucial. Here are the essential filing guidelines:
-
The form must be submitted within 60 days after your coverage termination.
-
Consider the consequences of late filing, which may result in loss of coverage.
-
You can submit the form via mail or online platforms like pdfFiller.
-
Utilize tracking methods for both mail and online submissions to confirm receipt.
Adhering to these guidelines will ensure that your application is processed without unnecessary delays, allowing you to maintain your health insurance coverage smoothly.
What Happens After You Submit the COBRA Election Form?
After submitting the COBRA Election Form, applicants can expect several follow-up actions. Initially, it's important to confirm the receipt of your application. This confirmation is crucial for peace of mind and ensures that your application is in process.
Typically, you can expect a response regarding your application within a specified timeframe, as outlined by the plan administrator. If additional information or clarification is needed, be prepared to follow up promptly to avoid delays in your coverage.
Security and Compliance for the COBRA Election Form
Handling sensitive information through the COBRA Election Form requires a focus on security and compliance. Platforms like pdfFiller implement robust security measures, including 256-bit encryption to safeguard your data. It is also compliant with regulations such as HIPAA and GDPR, ensuring your personal information is protected at all times.
Understanding these security features helps applicants feel confident when filling out and submitting the COBRA Election Form online, knowing their information is handled with the utmost care.
Get Started with pdfFiller to Complete Your COBRA Election Form
Using pdfFiller for completing your COBRA Election Form can greatly enhance the efficiency of your filing process. The platform offers extensive features, including the ability to edit and eSign documents easily.
Many users praise pdfFiller for its reliability and user-friendly interface, making it a preferred choice for those needing to complete the COBRA Election Form. By leveraging these services, you can streamline your form-filling experience and ensure all necessary details are accurately captured.
How to fill out the cobra election form
-
1.To access the COBRA Election Form on pdfFiller, visit the pdfFiller website and use the search bar to find the form by its name.
-
2.Once located, click on the form to open it in the pdfFiller editor.
-
3.Review the form to familiarize yourself with its layout and required fields before starting to fill it in.
-
4.Gather necessary information including your personal details, the qualifying event dates, and dependents' information to have at hand.
-
5.Begin filling out the form in the specified fields prominently marked, such as 'Employee Name' and qualifying event details.
-
6.Utilize the available tools on pdfFiller to add text into the blank fields, check appropriate boxes, and navigate the document smoothly.
-
7.After completing the required fields, review all the provided information to ensure accuracy before finalizing your submission.
-
8.Once you are satisfied, choose the save option to keep a copy of the completed form.
-
9.Download the form if you wish to have a local copy or submit it directly according to the instructions provided, ensuring it reaches the Trust Administrator on time.

Who is eligible to use the COBRA Election Form?
Individuals who have experienced a qualifying event, such as job loss or reduced hours, that affects their health insurance coverage are eligible to use the COBRA Election Form to elect continuation coverage.
What is the deadline for submitting the COBRA Election Form?
The form must be submitted to the Trust Administrator within 60 days after health coverage termination or from the date the employer provides the form, whichever is later.
How should the COBRA Election Form be submitted?
The completed COBRA Election Form should be submitted directly to the Trust Administrator as specified in the form’s instructions. Make sure to check for submission methods such as mail or electronic options.
Are there any supporting documents required with this form?
Typically, no additional documents are required with the COBRA Election Form. However, it’s advisable to have proof of the qualifying event handy for any future inquiries.
What are common mistakes to avoid when filling out the form?
Common mistakes include missing signatures, incorrect personal information, and failing to meet submission deadlines. Double-check all fields and ensure you review the form carefully before submission.
How long does it take to process the COBRA Election Form?
Processing times may vary based on the administrator's workload. Generally, it can take several days to a week to confirm COBRA election and coverage if the form is submitted correctly.
What if I need changes made to the COBRA Election Form after submission?
If changes are necessary after submission, it's crucial to contact the Trust Administrator immediately to discuss potential amendments or corrections.
Related Content
Related Forms




Related Catalogs
If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.