Aflac S00223 2008 free printable template
Show details
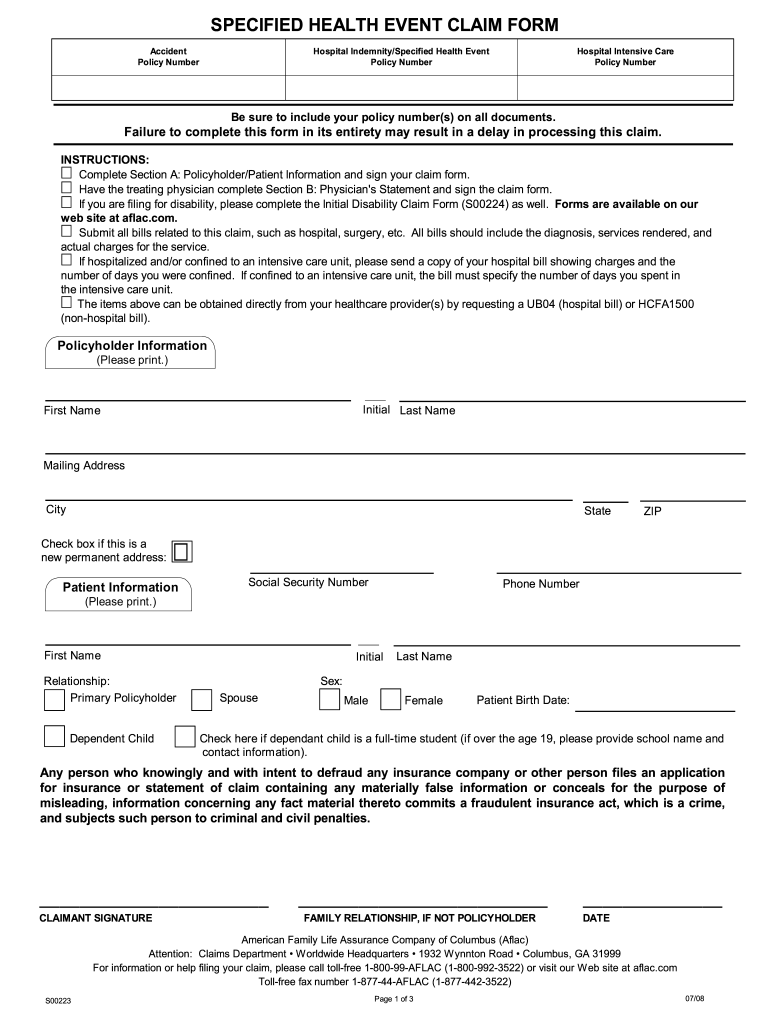
SPECIFIED HEALTH EVENT CLAIM FORM Accident Policy Number Hospital Indemnity/Specified Health Event Be sure to include your policy number s on all documents. Failure to complete this form in its entirety may result in a delay in processing this claim. INSTRUCTIONS Complete Section A Policyholder/Patient Information and sign your claim form. Have the treating physician complete Section B Physician s Statement and sign the claim form. If you are fil...
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign Aflac S00223
Edit your Aflac S00223 form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your Aflac S00223 form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit Aflac S00223 online



Follow the steps below to use a professional PDF editor:
1
Register the account. Begin by clicking Start Free Trial and create a profile if you are a new user.
2
Upload a document. Select Add New on your Dashboard and transfer a file into the system in one of the following ways: by uploading it from your device or importing from the cloud, web, or internal mail. Then, click Start editing.
3
Edit Aflac S00223. Text may be added and replaced, new objects can be included, pages can be rearranged, watermarks and page numbers can be added, and so on. When you're done editing, click Done and then go to the Documents tab to combine, divide, lock, or unlock the file.
4
Get your file. Select your file from the documents list and pick your export method. You may save it as a PDF, email it, or upload it to the cloud.
pdfFiller makes dealing with documents a breeze. Create an account to find out!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
Aflac S00223 Form Versions
Version
Form Popularity
Fillable & printabley
How to fill out Aflac S00223
How to fill out Aflac S00223
01
Gather necessary documents: Ensure you have your personal information, claim details, and any relevant medical records.
02
Obtain the Aflac S00223 form: Download it from the Aflac website or request it from your agent.
03
Fill in personal information: Complete your name, address, phone number, and policy number at the top of the form.
04
Provide claim details: Specify the type of claim you are filing and include dates of service or incident.
05
Include medical provider information: Enter the name and contact details of the healthcare provider treating you.
06
Sign and date the form: Ensure you sign and date where indicated to validate your claim.
07
Submit the form: Send the completed form to the designated Aflac claims department via mail or online upload.
Who needs Aflac S00223?
01
Individuals who have an Aflac insurance policy and need to file a claim for covered injuries or illnesses.
02
Policyholders seeking to receive benefits for hospital stays, surgical procedures, or other eligible medical expenses.
Fill
form
: Try Risk Free
People Also Ask about
What form do I need for Aflac claim?
UB04 (itemized hospital bill). ER report or operative report. (Please obtain the supporting documents for the corresponding benefit.)
Where to fax Aflac claim forms?
Fax this form to 1-877-442-3522 or return the form to Aflac, Attn: Claims Department, Worldwide Headquarters, 1932 Wynnton Road, Columbus, GA 31999, as soon as possible in order to expedite claim review.
What form does Aflac need to submit a claim?
UB04 (itemized hospital bill). ER report or operative report. (Please obtain the supporting documents for the corresponding benefit.)
What is a UB 04 form for Aflac?
Itemized hospital bill (IHB). UB04 (itemized hospital bill). ER visit. (Please obtain the supporting documents for the corresponding benefit.)
What is the UB 04 claim form?
The CMS-1450 form (aka UB-04 at present) can be used by an institutional provider to bill a Medicare fiscal intermediary (FI) when a provider qualifies for a waiver from the Administrative Simplification Compliance Act (ASCA) requirement for electronic submission of claims.
What is a specified health event?
Aflac Specified Health Event Protection is designed to provide you with cash benefits if you experience a catastrophic event, such as a heart attack or stroke.
Why would Aflac deny a claim?
When Aflac denies your claim, they must provide you with the reason. The main reason why they will deny your claim is they do not think you meet the plan's definition of disabled.
What is a specified health policy?
Except as otherwise provided in this section, the term "specified health insurance policy" means any accident or health insurance policy (including a policy under a group health plan) issued with respect to individuals residing in the United States.
What information do I need to file an Aflac claim?
Policyholder's address. Date and description of injury. Location of the injury. Patient's name and date of birth.
What is Aflac specified disease lump sum?
Specified Disease Lump Sum Benefit Overview BUILDING BENEFIT Up to $500, accrued annually This benefit is payable one time per covered person, per lifetime. See policy for additional benefit details.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I edit Aflac S00223 from Google Drive?
By integrating pdfFiller with Google Docs, you can streamline your document workflows and produce fillable forms that can be stored directly in Google Drive. Using the connection, you will be able to create, change, and eSign documents, including Aflac S00223, all without having to leave Google Drive. Add pdfFiller's features to Google Drive and you'll be able to handle your documents more effectively from any device with an internet connection.
How can I send Aflac S00223 for eSignature?
To distribute your Aflac S00223, simply send it to others and receive the eSigned document back instantly. Post or email a PDF that you've notarized online. Doing so requires never leaving your account.
How do I complete Aflac S00223 on an Android device?
Use the pdfFiller app for Android to finish your Aflac S00223. The application lets you do all the things you need to do with documents, like add, edit, and remove text, sign, annotate, and more. There is nothing else you need except your smartphone and an internet connection to do this.
What is Aflac S00223?
Aflac S00223 is a form used by Aflac to report information regarding claims for benefits under insurance policies.
Who is required to file Aflac S00223?
Individuals or entities who are filing claims for Aflac insurance benefits are required to file Aflac S00223.
How to fill out Aflac S00223?
To fill out Aflac S00223, provide all required personal and policy information, details of the claim, supporting documentation, and sign the form where indicated.
What is the purpose of Aflac S00223?
The purpose of Aflac S00223 is to facilitate the claims process by gathering necessary information for assessing and processing Aflac insurance claims.
What information must be reported on Aflac S00223?
The information that must be reported on Aflac S00223 includes the claimant's personal details, policy number, date of loss, description of the claim, and any relevant medical or supporting documents.
Fill out your Aflac S00223 online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Aflac s00223 is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms







If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
