Medical Claim Form






What is a Medical claim form?
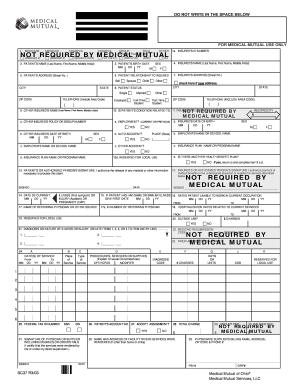
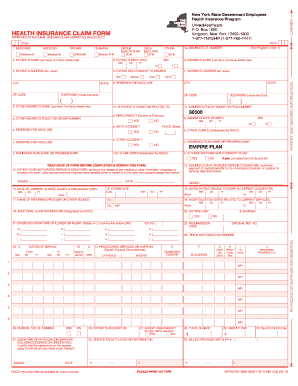
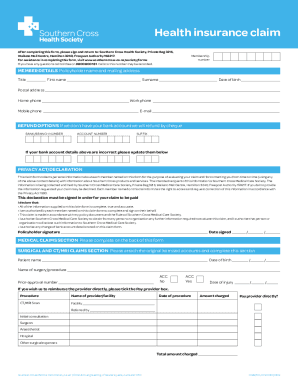
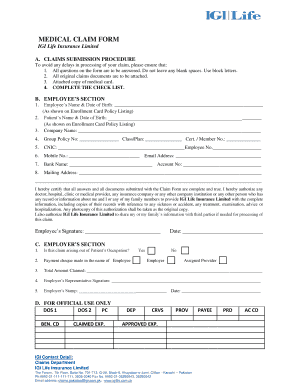
A Medical claim form is a document used to request reimbursement for healthcare services provided. It contains essential information such as patient details, diagnosis, treatment received, and costs incurred.
What are the types of Medical claim form?
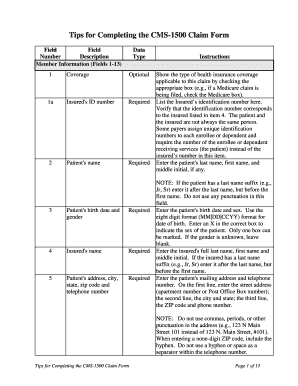
There are different types of Medical claim forms based on the insurance provider and the type of healthcare service. Some common types include: 1. CMS-1500: Used for physician and outpatient services 2. UB-04: Used for hospital claims 3. Dental claim form: Used for dental services 4. Prescription drug claim form: Used for medication expenses
How to complete Medical claim form?
Completing a Medical claim form accurately is crucial to ensure timely reimbursement. Here are some steps to help you fill out the form correctly:
pdfFiller empowers users to create, edit, and share documents online. Offering unlimited fillable templates and powerful editing tools, pdfFiller is the only PDF editor you need to get your documents done.