HHS Form CMS-20027 2010 free printable template
Show details
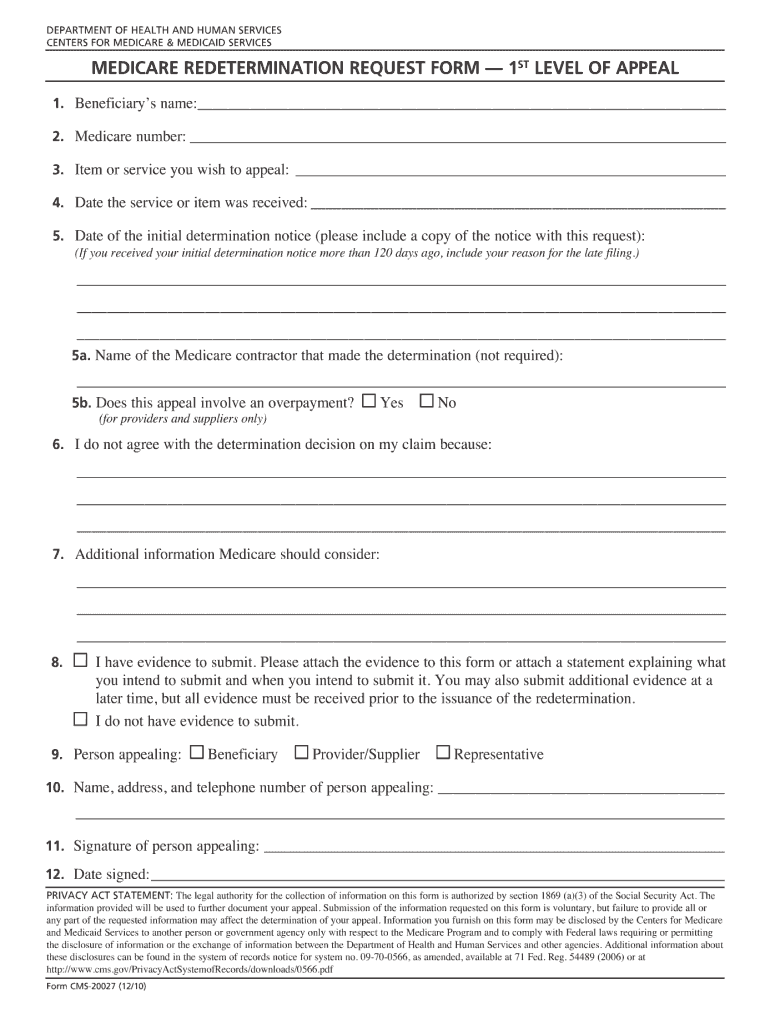
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES medicare redetermination request form -- 1st Level of appeal 1. Beneficiary's name: 2. Medicare number: 3. Item or
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign HHS Form CMS-20027
Edit your HHS Form CMS-20027 form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your HHS Form CMS-20027 form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing HHS Form CMS-20027 online



Here are the steps you need to follow to get started with our professional PDF editor:
1
Check your account. If you don't have a profile yet, click Start Free Trial and sign up for one.
2
Prepare a file. Use the Add New button to start a new project. Then, using your device, upload your file to the system by importing it from internal mail, the cloud, or adding its URL.
3
Edit HHS Form CMS-20027. Replace text, adding objects, rearranging pages, and more. Then select the Documents tab to combine, divide, lock or unlock the file.
4
Save your file. Select it from your list of records. Then, move your cursor to the right toolbar and choose one of the exporting options. You can save it in multiple formats, download it as a PDF, send it by email, or store it in the cloud, among other things.
It's easier to work with documents with pdfFiller than you could have believed. You may try it out for yourself by signing up for an account.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
HHS Form CMS-20027 Form Versions
Version
Form Popularity
Fillable & printabley
How to fill out HHS Form CMS-20027
How to fill out HHS Form CMS-20027
01
Obtain HHS Form CMS-20027 from the official HHS website or relevant office.
02
Review the instructions provided with the form to understand the requirements.
03
Fill out your personal information, including your name, address, and contact details in the designated sections.
04
Provide any required identification numbers, such as Social Security Number or Medicare Number, in the appropriate fields.
05
Answer all questions accurately, ensuring that you provide truthful and complete information.
06
Review the completed form for any errors or omissions before submission.
07
Sign and date the form where indicated to certify that the information is correct.
08
Submit the form according to the instructions, either electronically or by mailing it to the appropriate address.
Who needs HHS Form CMS-20027?
01
Individuals applying for health insurance coverage or benefits under Medicare or Medicaid programs.
02
Providers and organizations seeking reimbursement or funding related to health services.
03
Anyone affected by changes in health coverage or seeking support under specific health initiatives.
Fill
form
: Try Risk Free
People Also Ask about
What is form CMS L40D?
CMS-L40D Only beneficiaries who receive the general enrollment period (GEP) mailing from CMS can use Form CMS-L40D to enroll in SMI during the GEP. CMS mails Form CMS-L40D to individuals that refused, withdrew, or terminated SMI during the prior year. The beneficiary completes the Form CMS-L40D and sends it to CMS.
What is a CMS 1490S form?
DEPARTMENT OF HEALTH AND HUMAN SERVICES. CENTERS FOR MEDICARE & MEDICAID SERVICES. Form Approved OMB.
What is the purpose of the standard CMS 1500 claim form?
The CMS-1500 form is the standard claim form used by a non-institutional provider or supplier to bill Medicare carriers and durable medical equipment regional carriers (DMERCs) when a provider qualifies for a waiver from the Administrative Simplification Compliance Act (ASCA) requirement for electronic submission of
What is a CMS l564 form for?
This form is used for proof of group health care coverage based on current employment. This information is needed to process your Medicare enrollment application. The employer that provides the group health plan coverage completes the information about your health care coverage and dates of employment.
What is a form 40 B for Medicare?
This form is your application for Medicare Part B (Medical Insurance). You can use this form to sign up for Part B: During your Initial Enrollment Period (IEP) when you're first eligible for Medicare. During the General Enrollment Period (GEP) from January 1 through March 31 of each year.
What is Medicare form CMS 1490S?
SEND ONLY THE COMPLETED FORM TO YOUR MEDICARE ADMINISTRATIVE CONTRACTOR – Include a copy of the itemized bill and any supporting documents. Make a copy of your claim submission for your records and allow at least 60 days for Medicare to receive and process your request.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I send HHS Form CMS-20027 for eSignature?
Once your HHS Form CMS-20027 is ready, you can securely share it with recipients and collect eSignatures in a few clicks with pdfFiller. You can send a PDF by email, text message, fax, USPS mail, or notarize it online - right from your account. Create an account now and try it yourself.
How do I make edits in HHS Form CMS-20027 without leaving Chrome?
Install the pdfFiller Google Chrome Extension in your web browser to begin editing HHS Form CMS-20027 and other documents right from a Google search page. When you examine your documents in Chrome, you may make changes to them. With pdfFiller, you can create fillable documents and update existing PDFs from any internet-connected device.
Can I create an electronic signature for signing my HHS Form CMS-20027 in Gmail?
You may quickly make your eSignature using pdfFiller and then eSign your HHS Form CMS-20027 right from your mailbox using pdfFiller's Gmail add-on. Please keep in mind that in order to preserve your signatures and signed papers, you must first create an account.
What is HHS Form CMS-20027?
HHS Form CMS-20027 is a form used by healthcare providers to report information related to quality improvement and patient safety programs.
Who is required to file HHS Form CMS-20027?
Healthcare providers and organizations that participate in Medicare or Medicaid programs and are involved in quality improvement initiatives are required to file HHS Form CMS-20027.
How to fill out HHS Form CMS-20027?
To fill out HHS Form CMS-20027, providers should provide accurate information regarding their quality improvement initiatives, including details on program objectives, activities conducted, and outcomes achieved. Be sure to follow the form's instructions closely.
What is the purpose of HHS Form CMS-20027?
The purpose of HHS Form CMS-20027 is to collect data on quality improvement efforts to facilitate assessment and improvement in healthcare delivery and patient outcomes.
What information must be reported on HHS Form CMS-20027?
HHS Form CMS-20027 requires reporting of various information, including specific quality improvement initiatives, goals of the initiatives, methods employed, results obtained, and data supporting the outcomes.
Fill out your HHS Form CMS-20027 online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
HHS Form CMS-20027 is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms






If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
