Last updated on May 4, 2026
HHS Form CMS-20027 2010 free printable template
pdfFiller is not affiliated with any government organization

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
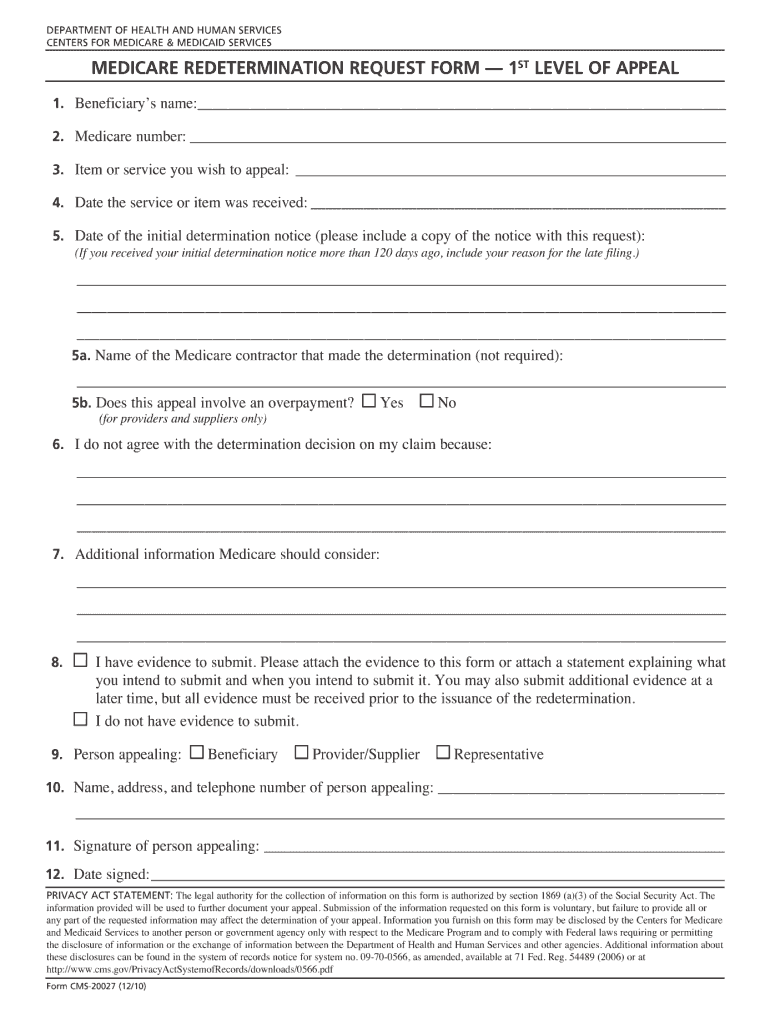
What is HHS Form CMS-20027
The HHS Form CMS-20027 is a document used by health care providers to report potential or actual adverse events related to healthcare services for oversight purposes.
pdfFiller scores top ratings on review platforms
Who needs HHS Form CMS-20027?
Explore how professionals across industries use pdfFiller.

HHS Form CMS-20027 is needed by:
-
Healthcare providers submitting adverse event reports
-
Medical facilities involved in patient care
-
Public health officials monitoring safety
-
Regulatory agencies assessing compliance
-
Legal representatives managing patient safety cases
Comprehensive Guide to HHS Form CMS-20027
What is the HHS Form CMS-20027?
The HHS Form CMS-20027 is a critical healthcare form used primarily for documenting specific patient information and eligibility. Issued by the Department of Health and Human Services, this form plays a vital role in the healthcare sector by facilitating communication between providers and patients. Understanding the purpose of CMS-20027 helps ensure accurate and timely submissions in various healthcare processes.
Purpose and Benefits of Completing the HHS Form CMS-20027
The main objectives of the HHS Form CMS-20027 include the accurate collection of data essential for patient care and administrative operations. Completing the form correctly is beneficial as it not only streamlines healthcare processes but also enhances patient outcomes through proper record-keeping. Additionally, the timely submission of this form can significantly affect both patients and healthcare providers, ensuring seamless operation within the healthcare system.
Who Needs the HHS Form CMS-20027?
This form is primarily required by healthcare providers who need to gather pertinent information from patients. Individuals seeking medical care must also be aware of their eligibility for CMS-20027. Common scenarios that necessitate the use of this form include patient admissions, insurance claims, and compliance with healthcare regulations.
When to File the HHS Form CMS-20027
Filing deadlines for the HHS Form CMS-20027 are crucial for compliance and should not be overlooked. Typically, this form should be submitted as soon as eligibility criteria are met or during critical healthcare events. Late filing may result in delays in patient care or complications in claims processing, underscoring the importance of timely submissions.
How to Fill Out the HHS Form CMS-20027 Online (Step-by-Step)
Filling out the HHS Form CMS-20027 online can be easily accomplished using pdfFiller. Follow these steps:
-
Access pdfFiller and choose the CMS-20027 form.
-
Complete all required fields, ensuring accuracy.
-
Review any section that may require additional clarification.
-
Save your progress or submit once completed.
This step-by-step guide ensures users fill out HHS Form CMS-20027 online effectively, utilizing pdfFiller’s tools for a smooth experience.
Common Errors to Avoid When Filling Out the HHS Form CMS-20027
To minimize errors in the HHS Form CMS-20027, users should be conscious of frequently made mistakes, such as incorrect personal information or missed signatures. To prevent these, conduct a thorough review of the form before submission. Taking the time to check each section can save you from potential complications.
How to Submit the HHS Form CMS-20027
Submitting the HHS Form CMS-20027 can be done through various methods, including:
-
Online via pdfFiller for immediate processing.
-
Mail to the appropriate healthcare agency.
-
In-person submission at designated locations.
Be aware of any applicable fees and processing times associated with each submission method to ensure smooth handling of the form.
Security and Compliance When Filling Out the HHS Form CMS-20027
When filling out the HHS Form CMS-20027, understanding the security measures in place is essential. pdfFiller employs 256-bit encryption and adheres to SOC 2 Type II standards, ensuring data protection and compliance with regulations such as HIPAA. Users can trust that their sensitive information is handled securely throughout the form-filling process.
How pdfFiller Can Help with Completing the HHS Form CMS-20027
pdfFiller provides a range of capabilities that simplify the process of editing, filling, and eSigning the HHS Form CMS-20027. With user-friendly tools, pdfFiller allows for a more efficient form-filling experience, encouraging users to leverage these advantages to streamline their documentation efforts.
Completing Your HHS Form CMS-20027 with Confidence
Users are encouraged to take action and complete the HHS Form CMS-20027 confidently using pdfFiller’s intuitive tools. The platform offers support and resources for individuals who may need assistance in navigating the form, ensuring a smooth completion process.
How to fill out the HHS Form CMS-20027
-
1.Open your web browser and navigate to pdfFiller's website.
-
2.Search for HHS Form CMS-20027 in the form library or upload the file if you already have it.
-
3.Once the form is loaded, review the sections to familiarize yourself with the fields required.
-
4.Gather necessary information including patient identifiers, details of the event, and any relevant documentation.
-
5.Click on each field to enter your information, verifying that everything is accurately filled in.
-
6.If you make a mistake, utilize the erase tool to remove the text and re-enter the correct information.
-
7.After completing all sections of the form, look for a review option to double-check your entries for correctness.
-
8.Once reviewed, proceed to save the document by clicking on the save option; choose a format for download if needed.
-
9.Finally, submit the form through the platform as directed, or download and print it for submission via traditional methods.

What are the eligibility requirements for submitting HHS Form CMS-20027?
Eligibility to submit HHS Form CMS-20027 typically includes authorized healthcare professionals and organizations experiencing adverse events. Make sure to verify that your facility can report events relevant to patient care and safety.
Are there deadlines for submitting this form?
There are no standard deadlines specified for HHS Form CMS-20027; however, timely reporting of adverse events is crucial for patient safety and regulatory compliance. It's advisable to submit the form as soon as incidents occur.
How can I submit HHS Form CMS-20027?
HHS Form CMS-20027 can be submitted electronically through authorized platforms like pdfFiller or printed and sent via mail to the designated HHS office. Ensure to follow all guidelines for submission to maintain compliance.
What supporting documents do I need to include?
When submitting HHS Form CMS-20027, it's essential to include any relevant patient information, incident reports, and supporting documentation that can provide context for the reported adverse event.
What common mistakes should I avoid when filling out this form?
Common mistakes include incomplete fields, incorrect patient identifiers, and failing to attach supporting documents. Always double-check entries and ensure that all necessary information is provided before submission.
How long does it take to process HHS Form CMS-20027?
Processing times can vary depending on the volume of submissions and the complexity of the reported events. It’s generally advisable to expect a processing period of several weeks.
What if I have form-specific concerns?
For form-specific questions regarding HHS Form CMS-20027, consult the official guidelines provided by the HHS or reach out to their support. They provide detailed resources for assistance.
HHS Form CMS-20027 Form Versions
Related Content
Related Forms



Get the latest insights from our blog
If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.