Get the free My patient advocate has authority to consent to or refuse treatment on my - michigan...
Show details
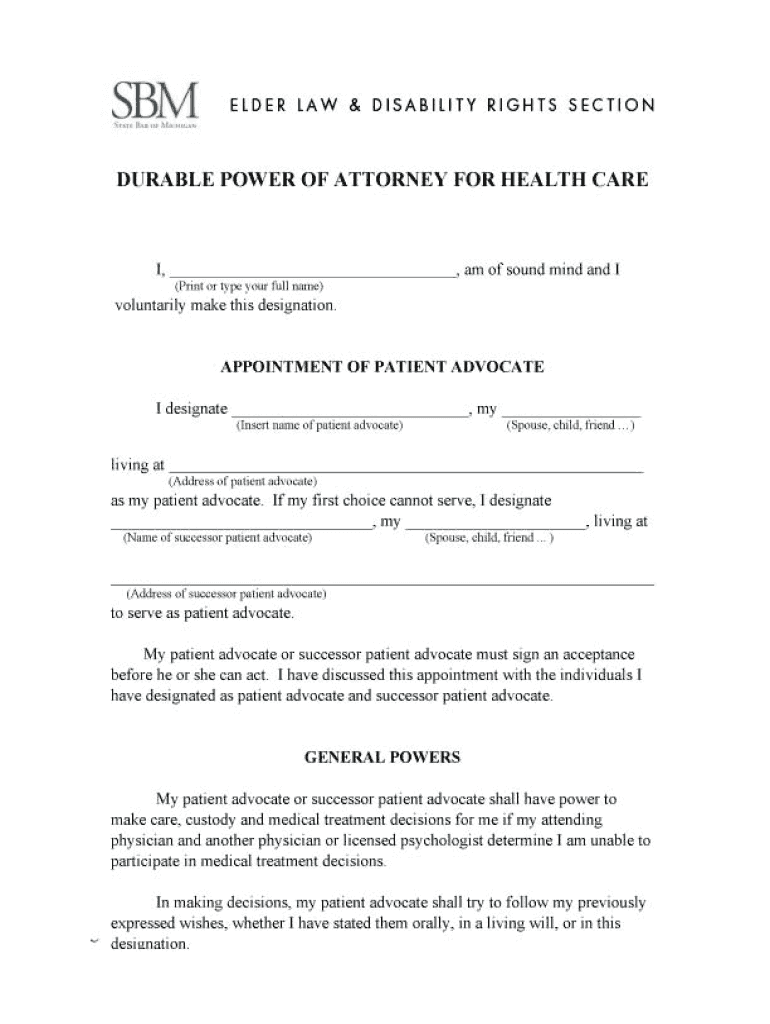
My patient advocate has authority to consent to or refuse treatment on my behalf, to arrange medical and personal services for me, including admission to a hospital or nursing care facility, and to
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign my patient advocate has
Edit your my patient advocate has form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your my patient advocate has form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing my patient advocate has online



Here are the steps you need to follow to get started with our professional PDF editor:
1
Log in to account. Start Free Trial and sign up a profile if you don't have one yet.
2
Prepare a file. Use the Add New button. Then upload your file to the system from your device, importing it from internal mail, the cloud, or by adding its URL.
3
Edit my patient advocate has. Rearrange and rotate pages, add and edit text, and use additional tools. To save changes and return to your Dashboard, click Done. The Documents tab allows you to merge, divide, lock, or unlock files.
4
Save your file. Select it from your records list. Then, click the right toolbar and select one of the various exporting options: save in numerous formats, download as PDF, email, or cloud.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out my patient advocate has
01
Start by gathering all the necessary information and documents required for filling out the patient advocate form. This may include personal identification documents, medical history, and contact information for your chosen advocate.
02
Carefully read through the instructions provided with the patient advocate form to ensure you understand the requirements and guidelines for filling it out.
03
Begin by filling out your personal information, including your full name, date of birth, address, and contact details. It is important to provide accurate and up-to-date information in this section.
04
Next, indicate the purpose of your patient advocate has. Provide details about why you feel the need for a patient advocate and what specific responsibilities or decisions you would like them to handle on your behalf.
05
If there is a specific individual you have chosen as your patient advocate, provide their full name, contact information, and their relationship to you. It is essential to discuss your decision with this person beforehand to ensure their willingness to take on this role.
06
If you have any special instructions or preferences regarding your healthcare, make sure to include them in the appropriate section of the form. For example, if you have certain religious or cultural considerations that should be taken into account, mention them here.
07
Review the completed form carefully to ensure all the information provided is accurate and complete. Double-check for any errors or omissions that may need to be corrected.
08
Sign and date the form in the designated spaces to certify that the information provided is true and accurate to the best of your knowledge.
09
Make copies of the completed form for your records and provide a copy to your chosen patient advocate. Additionally, it may be beneficial to inform your healthcare provider about your patient advocate has and provide them with a copy of the form for their records.
Who needs my patient advocate has?
01
Individuals who have ongoing medical conditions or chronic illnesses that may require future decision-making or medical care coordination.
02
Those who anticipate or are currently undergoing medical treatments, surgeries, or procedures that may involve complex decisions or potential complications.
03
Elderly individuals or those with declining cognitive function who may require assistance and advocacy in managing their healthcare.
04
People with disabilities who may require support in navigating the healthcare system and advocating for their specific needs.
05
Anyone who wishes to ensure their healthcare wishes and preferences are respected and followed, even if they are unable to communicate or make decisions for themselves.
Remember that the need for a patient advocate may vary depending on individual circumstances, so it is essential to assess your own situation and consult with healthcare professionals to determine if having a patient advocate is beneficial for you.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I manage my my patient advocate has directly from Gmail?
Using pdfFiller's Gmail add-on, you can edit, fill out, and sign your my patient advocate has and other papers directly in your email. You may get it through Google Workspace Marketplace. Make better use of your time by handling your papers and eSignatures.
How can I edit my patient advocate has from Google Drive?
pdfFiller and Google Docs can be used together to make your documents easier to work with and to make fillable forms right in your Google Drive. The integration will let you make, change, and sign documents, like my patient advocate has, without leaving Google Drive. Add pdfFiller's features to Google Drive, and you'll be able to do more with your paperwork on any internet-connected device.
How can I get my patient advocate has?
It’s easy with pdfFiller, a comprehensive online solution for professional document management. Access our extensive library of online forms (over 25M fillable forms are available) and locate the my patient advocate has in a matter of seconds. Open it right away and start customizing it using advanced editing features.
What is my patient advocate has?
Your patient advocate has the authority to make medical decisions on your behalf in case you are unable to do so.
Who is required to file my patient advocate has?
You or your legal representative are required to file your patient advocate form.
How to fill out my patient advocate has?
You can fill out your patient advocate form by providing your personal information, selecting your advocate, and signing the form.
What is the purpose of my patient advocate has?
The purpose of your patient advocate form is to ensure that your medical wishes are respected and carried out when you are unable to communicate them yourself.
What information must be reported on my patient advocate has?
Your patient advocate form must include your personal details, the selected advocate, and any specific medical wishes or instructions.
Fill out your my patient advocate has online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
My Patient Advocate Has is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms




If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
