Last updated on Mar 23, 2026
Get the free Prior Authorization Criteria Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
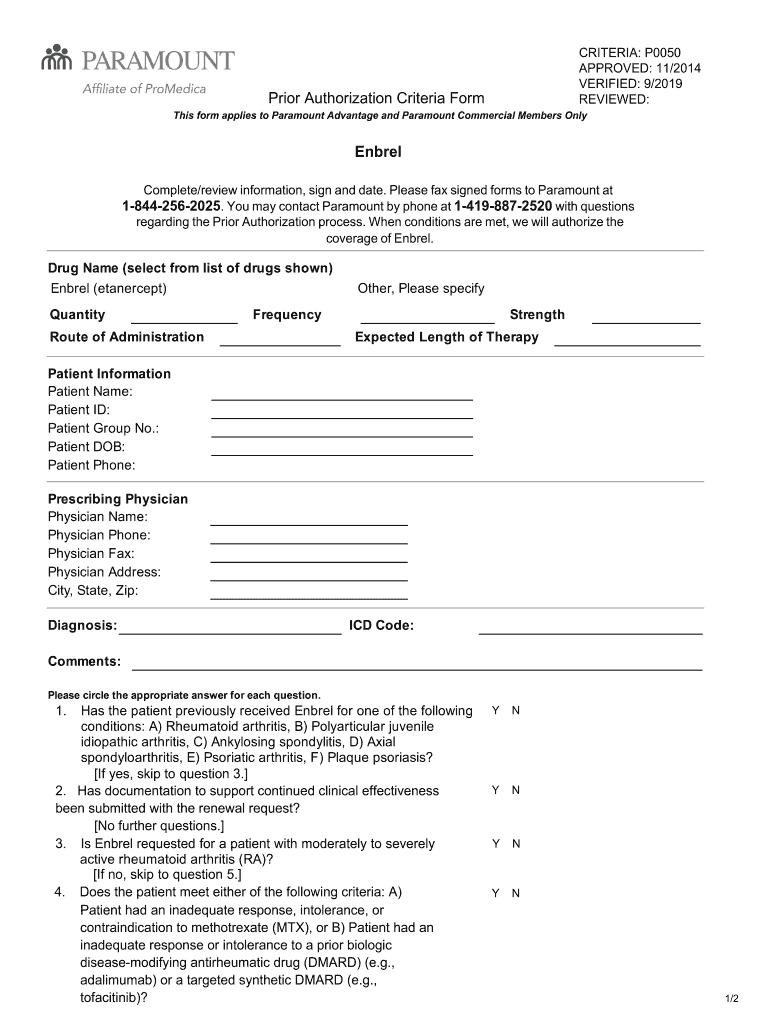
What is prior authorization criteria form
The Prior Authorization Criteria Form is a healthcare document used by providers to request approval for the drug Enbrel for specific medical conditions.
pdfFiller scores top ratings on review platforms
Who needs prior authorization criteria form?
Explore how professionals across industries use pdfFiller.

Prior authorization criteria form is needed by:
-
Healthcare providers looking to prescribe Enbrel.
-
Patients requiring authorization for Enbrel treatment.
-
Pharmacists verifying medication approvals.
-
Insurance agents assessing claims for Enbrel prescriptions.
-
Clinical staff managing patient records and treatments.
Comprehensive Guide to prior authorization criteria form
What is the Prior Authorization Criteria Form?
The Prior Authorization Criteria Form is a critical document used in healthcare settings, enabling providers to request approval for specific medications, including Enbrel. This form facilitates communication between healthcare providers and insurance companies to ensure timely treatment for patients. It requires detailed information about the patient and their medical condition, which is vital for providers seeking drug approvals.
Essentially, the form outlines the necessary details that healthcare providers must submit, including patient information, diagnosis codes, and answers to clinical criteria questions. This approach helps streamline the prior authorization process and minimizes delays in patient treatment.
Purpose and Benefits of the Prior Authorization Criteria Form
The Prior Authorization Criteria Form serves several key functions that are essential for prescribers. Firstly, it aids in securing insurance approvals for medications like Enbrel, ensuring that patients can receive their prescribed treatment. Secondly, by adhering to clinical criteria for authorization, this form promotes compliance with necessary healthcare regulations.
Additionally, the efficient completion of this form significantly reduces delays in patient treatment, expediting the authorization process. This efficiency is particularly beneficial in urgent medical situations where timely approval is necessary for patient care.
Who Needs the Prior Authorization Criteria Form?
This form must be completed by healthcare providers and prescribers involved in patient care. It targets professionals who prescribe Enbrel and need prior authorization for their patients. Specifically, the form caters to patients who meet the clinical criteria for Enbrel candidature, allowing these patients access to necessary treatments.
Situations that necessitate the completion of this form include cases where a healthcare provider has determined that Enbrel is medically appropriate for a patient’s condition, requiring authorization for the treatment plan to proceed.
How to Fill Out the Prior Authorization Criteria Form Online
Filling out the Prior Authorization Criteria Form online is a straightforward process. The first step is to access the form through pdfFiller, where users can edit and complete the document digitally. Below is a guide to completing the form:
-
Log into your pdfFiller account and locate the Prior Authorization Criteria Form.
-
Complete each field with accurate patient and physician information.
-
Include relevant diagnosis codes and answer all required clinical criteria questions.
-
Review the form thoroughly to ensure all information is accurate and complete.
-
Finalize your form by applying the necessary signature.
These steps will help ensure that the form is filled out correctly, which is crucial for a successful submission.
Required Documents and Information to Include
When submitting the Prior Authorization Criteria Form, certain documentation and information are essential for a successful authorization request. Providers must include:
-
Patient’s complete medical history and relevant diagnosis codes.
-
Physician's details, including contact information and prescribing credentials.
-
Any supporting documents that substantiate the need for Enbrel, such as lab results or previous treatment notes.
Ensuring comprehensive information helps prevent delays in processing the authorization request. Incomplete submissions can lead to requests being put on hold, delaying patient treatment.
Submission Methods and What Happens After You Submit
After completing the Prior Authorization Criteria Form, it must be submitted correctly to ensure timely processing. Healthcare providers can fax the completed form to Paramount for review. This method ensures that it reaches the appropriate department efficiently.
Upon submission, providers can expect to receive authorization decisions typically within a specified timeframe based on the payer’s guidelines. If the authorization is denied or if additional information is required, follow-up actions will be necessary to resolve any outstanding issues or concerns related to the submission.
Common Errors and How to Avoid Them
Completing the Prior Authorization Criteria Form can lead to misunderstandings if common errors are made. Some frequent pitfalls include:
-
Missing or incorrect patient information that can result in processing delays.
-
Omitting necessary supporting documents that validate the authorization request.
-
Failing to double-check field entries before submission.
To avoid these issues, healthcare providers can use a validation checklist to confirm that every field is filled out correctly before submission. This proactive approach enhances accuracy and increases the chances of approval.
Security and Compliance for the Prior Authorization Criteria Form
Security and compliance are paramount when handling the Prior Authorization Criteria Form. Using pdfFiller, providers benefit from robust security measures, including 256-bit encryption, ensuring that sensitive patient information is protected during the authorization process. Adherence to HIPAA regulations is also a critical component for safeguarding patient privacy.
Understanding these security measures is essential when submitting forms electronically, as it reinforces the responsibility healthcare providers have in protecting patient data throughout the authorization process.
How pdfFiller Simplifies the Prior Authorization Process
pdfFiller plays a pivotal role in simplifying the Prior Authorization Criteria Form process. The platform offers various features that allow users to fill, edit, and eSign documents effortlessly. These capabilities contribute to a more manageable workflow for healthcare professionals, streamlining communication and document handling.
By utilizing pdfFiller, healthcare providers can benefit from the ease of access, enhanced security, and improved efficiency. Testimonials frequently highlight how pdfFiller has positively impacted the workflows of healthcare professionals, further illustrating its value in the prior authorization process.
Sample or Example of a Completed Prior Authorization Criteria Form
Providing users with a visual reference, a sample of a completed Prior Authorization Criteria Form can be invaluable. This example offers a clear representation of how to fill out the form correctly, including key sections that require attention.
Annotations can be helpful in clarifying the purpose of different fields, guiding users in replicating the form accurately. Users can utilize pdfFiller’s tools to create a similar form by following the demonstrated example, further enhancing their understanding of the submission process.
How to fill out the prior authorization criteria form
-
1.To begin, access the Prior Authorization Criteria Form on pdfFiller by searching it directly from the platform’s homepage or using the link provided by your healthcare facility.
-
2.Once the form is open, familiarize yourself with the layout, which includes multiple fillable fields, checkboxes, and instructions to guide you through the process.
-
3.Before filling out the form, gather all necessary data, such as patient information (name, age, and insurance details), physician's information, diagnosis codes, and any clinical criteria specifics related to Enbrel.
-
4.Start by entering the patient’s personal and insurance information in the designated fields. Ensure all information is accurate and up-to-date.
-
5.Next, fill in the prescriber’s details, including name, contact information, and any relevant identifiers required by the insurance provider.
-
6.Proceed to provide the diagnosis codes and articulate the medical condition or reasons for requesting Enbrel. Be thorough in answering all clinical criteria inquiries to avoid delays in approval.
-
7.After completing all fields, double-check each section for accuracy. You can use the review features in pdfFiller to highlight any overlooked areas or missing information.
-
8.Once you're confident that the form is complete and accurate, proceed to sign the document electronically as required. Make sure to obtain the necessary signatures before submission.
-
9.Finally, save your work by downloading a copy of the completed form. You can also choose to submit the form directly through pdfFiller via fax to Paramount for review.

Who needs to fill out the Prior Authorization Criteria Form?
The form must be filled out by healthcare providers prescribing Enbrel for a patient to obtain authorization from the insurance company. It is also crucial for pharmacists and clinical staff managing patient information.
What information do I need to complete the form?
You'll need the patient's personal details, insurance information, physician’s data, relevant diagnosis codes, and answers to clinical criteria inquiries specific to Enbrel.
How do I submit the completed form?
After completing the form on pdfFiller, you can submit it by faxing it directly to Paramount, as indicated on the form. Make sure that all required signatures are obtained before sending.
What should I do if I make a mistake on the form?
If you make a mistake while completing the Prior Authorization Criteria Form, you can easily correct it using pdfFiller's editing tools. Review all sections before finalizing the form.
Is there a deadline for submitting this form?
It’s important to submit the form as soon as possible to avoid delays in medication approval. Insurance companies typically have specific timelines for processing authorizations.
Are there any fees associated with submitting the form?
While there are generally no fees for submitting the Prior Authorization Criteria Form, it’s advisable to check with your insurance provider for any costs associated with authorization requests.
What happens after I submit the form?
Once submitted, the insurance company will review your request and determine whether to approve the prior authorization, which may take several days based on their processing times.
Related Forms



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.