CA DWC-AU-906 2000 free printable template
Show details
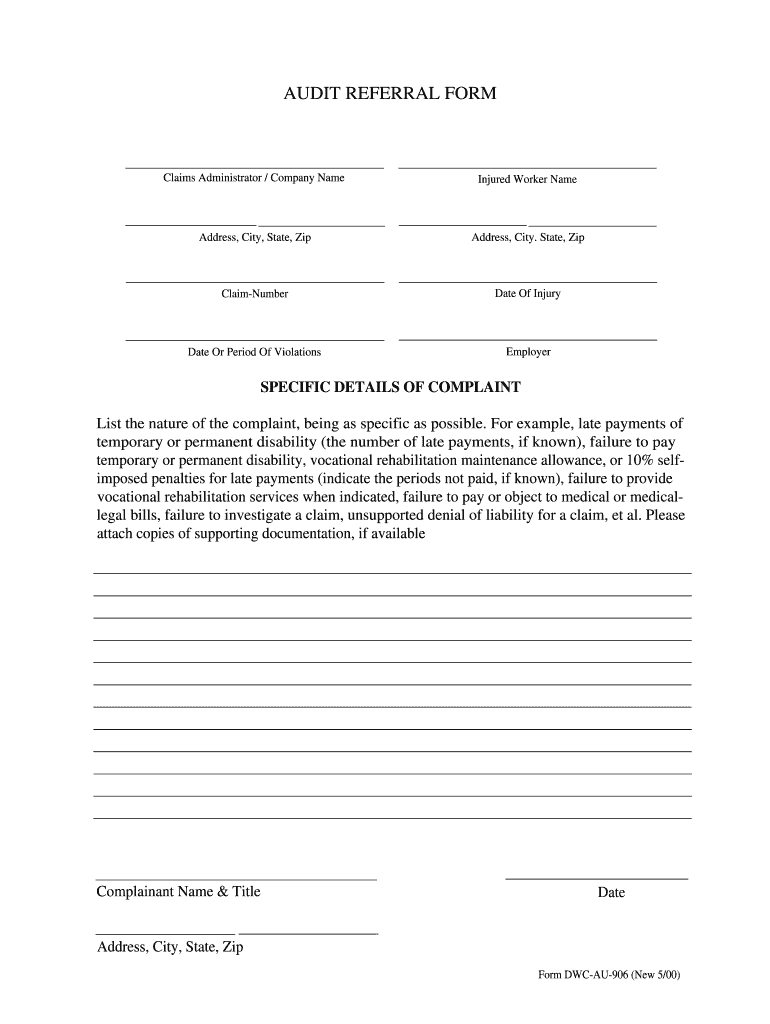
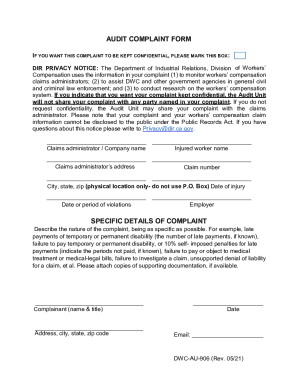
HOW TO FILE A COMPLAINT WITH THE AUDIT UNIT The Audit Unit of the Division of Workers' Compensation tracks complaints against workers' compensation claims administrators to help in determining which
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign CA DWC-AU-906
Edit your CA DWC-AU-906 form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your CA DWC-AU-906 form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing CA DWC-AU-906 online



Use the instructions below to start using our professional PDF editor:
1
Create an account. Begin by choosing Start Free Trial and, if you are a new user, establish a profile.
2
Prepare a file. Use the Add New button. Then upload your file to the system from your device, importing it from internal mail, the cloud, or by adding its URL.
3
Edit CA DWC-AU-906. Add and change text, add new objects, move pages, add watermarks and page numbers, and more. Then click Done when you're done editing and go to the Documents tab to merge or split the file. If you want to lock or unlock the file, click the lock or unlock button.
4
Get your file. When you find your file in the docs list, click on its name and choose how you want to save it. To get the PDF, you can save it, send an email with it, or move it to the cloud.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
CA DWC-AU-906 Form Versions
Version
Form Popularity
Fillable & printabley
How to fill out CA DWC-AU-906
How to fill out CA DWC-AU-906
01
Obtain the CA DWC-AU-906 form from the California Division of Workers' Compensation website.
02
Fill in the employer's information, including name, address, and contact details.
03
Provide the injured employee's information, including name, address, and date of injury.
04
Specify the type of injury or illness and any relevant medical information.
05
Indicate the amount of compensation requested and provide any supporting documentation.
06
Review the completed form for accuracy and completeness.
07
Sign and date the form to certify that the information provided is true and correct.
08
Submit the CA DWC-AU-906 form to the appropriate workers' compensation insurance carrier.
Who needs CA DWC-AU-906?
01
Employers who need to report a workers' compensation claim.
02
Injured employees seeking compensation for work-related injuries or illnesses.
03
Insurance companies processing claims for workers' compensation.
04
Legal representatives assisting with workers' compensation cases.
Fill
form
: Try Risk Free
People Also Ask about
What is a DWC-1 claim form?
Your DWC-1 claim form is your declaration that you have been injured while working, and that you believe you require compensation while you recover. A common misconception is that going to the doctor – something you should doas soon as possible – essentially creates a workers' comp claim for you.
Who completes DWC-1 form?
Your employer should fill out the “employer” section and forward the completed claim form to the insurance company. You should receive a copy of the completed claim form from your employer. If you don't, request a copy and keep it for your records.
What is the employer's wage statement DWC form 003?
The purpose of the form is to provide the employee's wage information to the carrier for calculating the employee's Average Weekly Wage (AWW) to establish benefits due to the employee or a beneficiary.
What is a DWC notice?
Division of Workers' Compensation Notice to Employees--Injuries Caused By Work. You may be entitled to workers' compensation benefits if you are injured or become ill because of your job. Workers' compensation covers most work-related physical or mental injuries and illnesses.
How to fill out a DWC-1 form?
Filling out a DWC-1 form is actually pretty straightforward.On the form, you will need to only fill out the “Employee” section, which asks for basic information: Name, date, and address. Date and location of injury. Brief description of injury. List of injured body parts. Social Security Number.
What is the purpose of the DWC-1 form?
DWC-1 Workers Compensation Claim Form. This is the form you will complete and send to EMPLOYERS to initiate the claim process for your employee. This form must be completed and provided to EMPLOYERS within one working day from you becoming aware of a work-related injury or occupational disease.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I send CA DWC-AU-906 for eSignature?
When you're ready to share your CA DWC-AU-906, you can send it to other people and get the eSigned document back just as quickly. Share your PDF by email, fax, text message, or USPS mail. You can also notarize your PDF on the web. You don't have to leave your account to do this.
How do I make edits in CA DWC-AU-906 without leaving Chrome?
Download and install the pdfFiller Google Chrome Extension to your browser to edit, fill out, and eSign your CA DWC-AU-906, which you can open in the editor with a single click from a Google search page. Fillable documents may be executed from any internet-connected device without leaving Chrome.
How do I fill out CA DWC-AU-906 on an Android device?
Complete CA DWC-AU-906 and other documents on your Android device with the pdfFiller app. The software allows you to modify information, eSign, annotate, and share files. You may view your papers from anywhere with an internet connection.
What is CA DWC-AU-906?
CA DWC-AU-906 is a form used in California for reporting information related to workers' compensation claims and the utilization review process.
Who is required to file CA DWC-AU-906?
Employers, workers' compensation insurers, or claims administrators are required to file CA DWC-AU-906 when there is a request for medical treatment authorization.
How to fill out CA DWC-AU-906?
To fill out CA DWC-AU-906, the filer must provide details such as the injured worker's information, the requested treatment, relevant medical history, and the justification for the treatment request.
What is the purpose of CA DWC-AU-906?
The purpose of CA DWC-AU-906 is to ensure that necessary medical treatments for injured workers are reviewed and authorized appropriately under California workers' compensation laws.
What information must be reported on CA DWC-AU-906?
CA DWC-AU-906 requires reporting information such as the injured employee's name and claim number, the requesting provider's details, the type of treatment requested, and any relevant medical documentation.
Fill out your CA DWC-AU-906 online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
CA DWC-AU-906 is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
