


What is Medical Claim Questionnaire.doc Form?
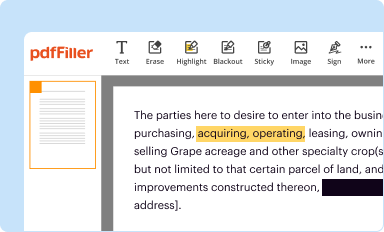
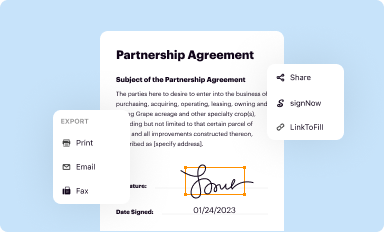
The Medical Claim Questionnaire.doc is a Word document needed to be submitted to the specific address in order to provide certain information. It needs to be completed and signed, which can be done manually, or via a certain software such as PDFfiller. This tool lets you complete any PDF or Word document directly in your browser, customize it depending on your needs and put a legally-binding electronic signature. Right away after completion, the user can easily send the Medical Claim Questionnaire.doc to the relevant person, or multiple recipients via email or fax. The blank is printable as well because of PDFfiller feature and options offered for printing out adjustment. In both electronic and in hard copy, your form will have a clean and professional look. It's also possible to turn it into a template for further use, there's no need to create a new document from the beginning. All you need to do is to edit the ready form.
Instructions for the form Medical Claim Questionnaire.doc
Before filling out Medical Claim Questionnaire.doc Word template, make sure that you prepared enough of necessary information. It's a very important part, as far as some typos can bring unwanted consequences from re-submission of the whole word form and filling out with missing deadlines and you might be charged a penalty fee. You have to be observative enough filling out the digits. At first glimpse, it might seem to be not challenging thing. Nevertheless, it is simple to make a mistake. Some people use some sort of a lifehack saving all data in a separate document or a record book and then attach it's content into document template. Anyway, put your best with all efforts and present valid and solid information with your Medical Claim Questionnaire.doc word form, and doublecheck it during the process of filling out all fields. If it appears that some mistakes still persist, you can easily make some more corrections when using PDFfiller editor and avoid blowing deadlines.
How to fill out Medical Claim Questionnaire.doc
In order to start filling out the form Medical Claim Questionnaire.doc, you need a template of it. When using PDFfiller for completion and filing, you can obtain it in several ways:
- Find the Medical Claim Questionnaire.doc form in PDFfiller’s filebase.
- You can also upload the template with your device in Word or PDF format.
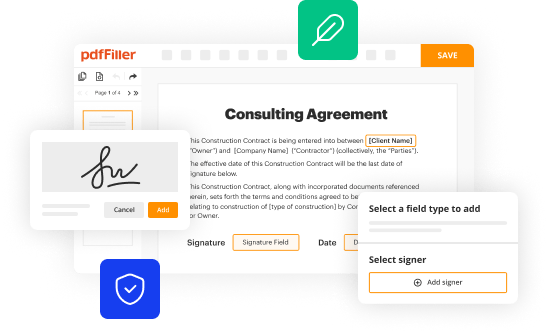
- Create the document all by yourself in creator tool adding all necessary object in the editor.
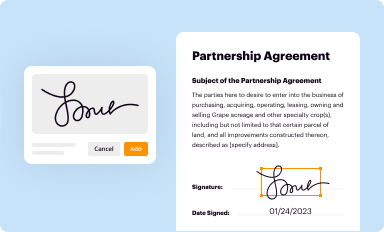
Whatever choise you make, you'll have all features you need for your use. The difference is, the template from the archive contains the required fillable fields, and in the rest two options, you will have to add them yourself. Nevertheless, this action is quite simple and makes your document really convenient to fill out. These fields can be easily placed on the pages, you can delete them as well. Their types depend on their functions, whether you are entering text, date, or place checkmarks. There is also a electronic signature field for cases when you want the word file to be signed by other people. You can sign it yourself via signing tool. Once you're good, all you have to do is press the Done button and proceed to the distribution of the form.