Get the free Coverage Determination Request Form
Show details
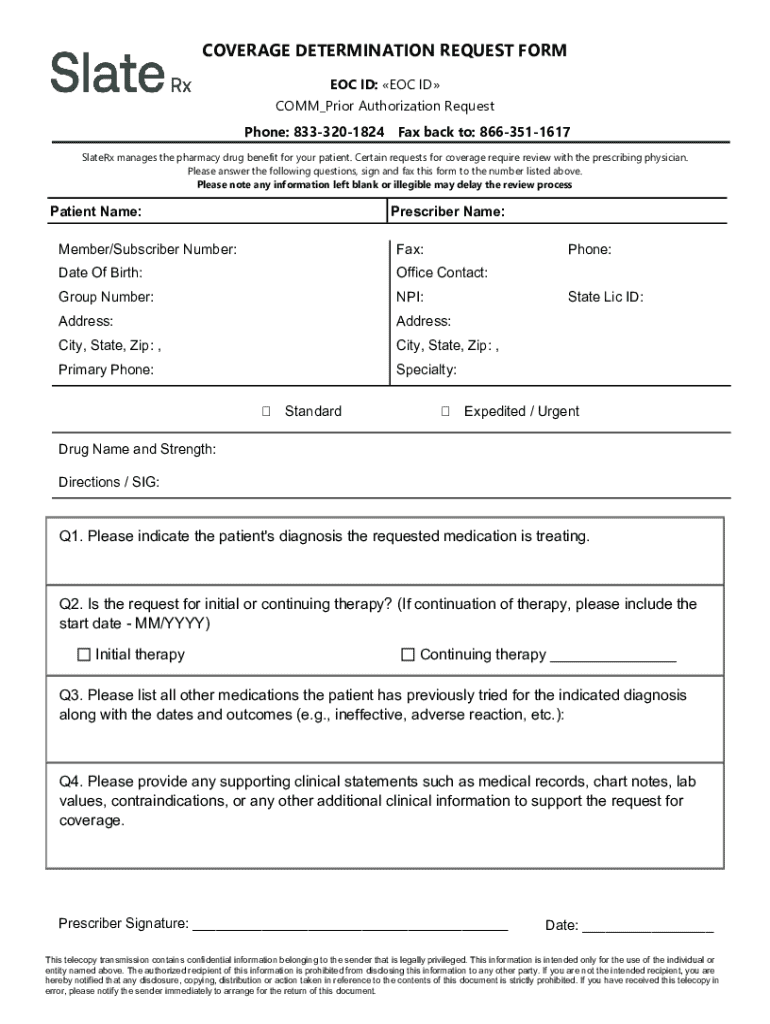
This form is used to request prior authorization for pharmacy drug benefits for patients, requiring details from both the patient and prescribing physician.
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign coverage determination request form
Edit your coverage determination request form form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your coverage determination request form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit coverage determination request form online



Use the instructions below to start using our professional PDF editor:
1
Set up an account. If you are a new user, click Start Free Trial and establish a profile.
2
Prepare a file. Use the Add New button. Then upload your file to the system from your device, importing it from internal mail, the cloud, or by adding its URL.
3
Edit coverage determination request form. Rearrange and rotate pages, insert new and alter existing texts, add new objects, and take advantage of other helpful tools. Click Done to apply changes and return to your Dashboard. Go to the Documents tab to access merging, splitting, locking, or unlocking functions.
4
Get your file. When you find your file in the docs list, click on its name and choose how you want to save it. To get the PDF, you can save it, send an email with it, or move it to the cloud.
With pdfFiller, it's always easy to work with documents. Try it out!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out coverage determination request form
How to fill out coverage determination request form
01
Gather necessary personal information including your name, address, phone number, and insurance details.
02
Provide details about your medical condition and the service or treatment you are requesting coverage for.
03
Include any relevant medical records or documentation supporting your request.
04
Fill out the sections of the form that ask for information about your healthcare provider.
05
Clearly state the reason for your request, including why the treatment is needed and any alternatives considered.
06
Review the completed form for accuracy and completeness.
07
Sign and date the form.
08
Submit the form according to your insurance company's guidelines, either online or by mail.
Who needs coverage determination request form?
01
Individuals who require specific medical treatments, services, or medications that are not automatically covered by their health insurance plan.
02
Patients seeking a review or appeal for denial of coverage from their insurance provider.
03
Healthcare providers submitting requests on behalf of their patients for medically necessary services.
A Comprehensive Guide to the Coverage Determination Request Form
Understanding the coverage determination request form
The coverage determination request form serves as a pivotal document in the healthcare landscape, particularly within the insurance process. It is primarily used by patients and healthcare providers to formally request coverage for specific treatments, medications, or procedures that may not be routinely covered under an insurance policy.
This form is essential because it provides a structured means for individuals to seek necessary healthcare services that are otherwise not included in their insurance plan. By submitting this form, patients can clarify their needs and justify why certain treatments should be covered, resulting in a smoother claims process.
Key components of the form
Details such as name, date of birth, and policy number.
Information about the healthcare provider making the request.
Specific details about the treatment, medication, or procedure requested.
Rationale for why the requested service is essential for the patient's health.
Who should use the coverage determination request form?
The target audience for the coverage determination request form is two-fold: patients and healthcare providers. Patients looking to cover specific treatments or medications that are not typically included in their insurance plans are the primary users of this document. Healthcare providers act as facilitators, helping patients navigate the complexities of insurance coverage and ensuring that all necessary information is accurately presented.
Using this form becomes necessary in various scenarios, such as when a patient's prescribed medication is deemed non-formulary by their insurance or when a certain procedure requires pre-authorization. Examples include requesting post-operative rehabilitation therapy or an experimental treatment not covered by an insurance policy.
Step-by-step guide to filling out the coverage determination request form
Step 1: Gather necessary information
Before filling out the form, make sure to gather relevant information. This includes the patient's medical history, details about the treatment or medication in question, and insurance policy information, such as the coverage terms and benefit exclusions. Comprehensive knowledge of existing medical records can bolster the request’s chances for approval.
Step 2: Completing the form accurately
Accuracy is critical when completing the coverage determination request form. Each section should be filled with attention to detail.
Fill in personal details including name, date of birth, and contact information.
Include the healthcare provider's name, contact number, and NPI number.
Provide detailed information about the treatment and its medical necessity.
Step 3: Reviewing your submission
Reviewing your submission is essential. Double-check for any errors that may invalidate your request. Common errors include misspelled names, incorrect dates or missing signatures. Ensuring the accuracy of the form can expedite processing and prevent unnecessary delays.
Submitting the coverage determination request form
The next crucial step after completing the coverage determination request form is submission. There are generally two accepted methods for submitting this document.
Most insurance companies provide a secure portal for online submissions which often speeds up the process.
For postal submissions, ensure that you follow specific guidelines such as including return addresses and proper postage.
After submission, it is wise to track your request. Following up with your insurer can keep you informed about the status of your coverage determination. The standard timelines for processing requests can vary, typically ranging from a few days to several weeks.
What happens after submission?
After submitting the coverage determination request form, it enters a review process where the insurance company evaluates the request based on the provided information and their coverage guidelines. This assessment involves checking the medical necessity and potential alternatives to the proposed treatment.
Possible outcomes of your request
There are generally two outcomes following the evaluation: - **Approval**: If your request is approved, you can proceed with the prescribed treatment knowing it is covered by your insurance. You should receive detailed instructions on how to proceed. - **Denial**: In the case of a denial, the insurance company must provide a clear explanation for the decision. Understanding your rights is crucial, as you may have options to appeal the denial.
Troubleshooting common issues
It’s not uncommon to face issues when submitting your coverage determination request form. Delays might arise from incomplete submissions or the need for additional information from your healthcare provider. To resolve these issues, maintain communication with the insurance company and seek feedback on any required changes.
Understanding denials
Denials can happen for various reasons. Common causes include insufficient medical evidence, treatments deemed experimental, or services outside of the coverage network. If you face a denial, it is your right to appeal the decision. Collect further documentation and consult with your healthcare provider to strengthen your appeal.
Resources for assistance
When navigating the coverage determination process, it’s beneficial to have supportive resources at hand. Many insurance providers have dedicated customer service teams that can assist with queries regarding the coverage determination request form.
Find contact numbers of customer service which can provide direct assistance.
Tap into local health advocacy groups that offer personalized support and guidance.
Utilize features like eSign and document editing capabilities to efficiently manage your form.
FAQs about the coverage determination request process
Understanding the coverage determination request form process often brings up several questions and concerns. For instance, if you find completion challenges, assistance can often be sought from healthcare providers or trained advocates. Furthermore, if a request is denied, it is indeed possible to appeal, and understanding the appeal process can empower you to seek the healthcare services you require.
Clarification on legal rights and procedures
Being aware of your legal rights within healthcare coverage determination is essential. Patients have the right to an appeal and should be informed about the procedures and timeframe for filing. Furthermore, insurers must provide you with the criteria used in making decisions. This transparency is critical for empowering patients in their healthcare journeys.
pdfFiller's role in simplifying the process
pdfFiller stands out as a powerful platform designed to streamline the entire process surrounding the coverage determination request form. Its tools allow users to seamlessly edit PDFs, eSign documents, and collaborate effectively on form management—all from a user-friendly, cloud-based environment. This capability significantly enhances the user experience by enabling flexibility and accessibility.
Benefits of using pdfFiller for coverage determination requests
The primary benefits of using pdfFiller include: - **Accessibility**: Forms can be accessed and completed from any device, making it convenient for both patients and providers. - **Collaboration**: Easily share documents among team members or with healthcare providers for quicker processing. - **eSigning**: Utilize the eSign feature to expedite form submission and enhance efficiency.
Latest news and updates
Staying informed on updates in healthcare policies and coverage determination is vital. Recently, Medicare has seen notable adjustments in its coverage policies, including increased provisions for telehealth services and updated guidelines on experimental treatments. Regularly checking informative articles and resources—like those available on pdfFiller—can ensure you remain knowledgeable and proactive in your healthcare decisions.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I manage my coverage determination request form directly from Gmail?
In your inbox, you may use pdfFiller's add-on for Gmail to generate, modify, fill out, and eSign your coverage determination request form and any other papers you receive, all without leaving the program. Install pdfFiller for Gmail from the Google Workspace Marketplace by visiting this link. Take away the need for time-consuming procedures and handle your papers and eSignatures with ease.
How do I edit coverage determination request form online?
pdfFiller allows you to edit not only the content of your files, but also the quantity and sequence of the pages. Upload your coverage determination request form to the editor and make adjustments in a matter of seconds. Text in PDFs may be blacked out, typed in, and erased using the editor. You may also include photos, sticky notes, and text boxes, among other things.
How do I fill out coverage determination request form on an Android device?
Complete coverage determination request form and other documents on your Android device with the pdfFiller app. The software allows you to modify information, eSign, annotate, and share files. You may view your papers from anywhere with an internet connection.
What is coverage determination request form?
The coverage determination request form is a document used to request an assessment of whether a specific health care service, medication, or treatment is covered under an individual's insurance plan.
Who is required to file coverage determination request form?
Typically, the coverage determination request form can be filed by the healthcare provider, the patient, or an authorized representative acting on behalf of the patient.
How to fill out coverage determination request form?
To fill out the coverage determination request form, the requester must provide detailed patient information, describe the treatment or service being requested, indicate the diagnosis, and include any supporting documents or medical necessity rationale.
What is the purpose of coverage determination request form?
The purpose of the coverage determination request form is to formally initiate a review process by the insurance provider to establish whether the requested service or medication is eligible for coverage under the patient's health plan.
What information must be reported on coverage determination request form?
The information that must be reported on the coverage determination request form typically includes the patient's demographic details, insurance policy number, the specific service or medication requested, diagnosis information, provider details, and medical documentation supporting the request.
Fill out your coverage determination request form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Coverage Determination Request Form is not the form you're looking for?Search for another form here.
Relevant keywords
If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
