Get the free Patient Reimbursement Request Form
Show details
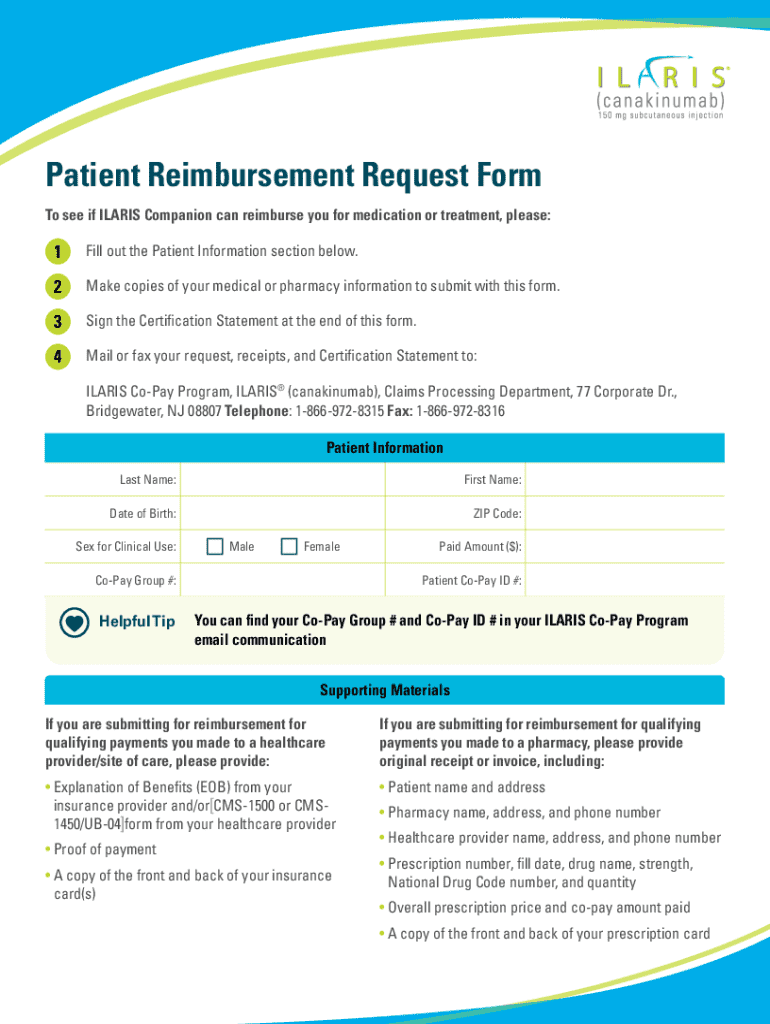
Patient Reimbursement Request Form To see if Companion can reimburse you for medication or treatment, please:1Fill out the Patient Information section below.2Make copies of your medical or pharmacy
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign patient reimbursement request form
Edit your patient reimbursement request form form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your patient reimbursement request form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing patient reimbursement request form online



Follow the steps below to benefit from the PDF editor's expertise:
1
Create an account. Begin by choosing Start Free Trial and, if you are a new user, establish a profile.
2
Prepare a file. Use the Add New button to start a new project. Then, using your device, upload your file to the system by importing it from internal mail, the cloud, or adding its URL.
3
Edit patient reimbursement request form. Rearrange and rotate pages, add new and changed texts, add new objects, and use other useful tools. When you're done, click Done. You can use the Documents tab to merge, split, lock, or unlock your files.
4
Save your file. Choose it from the list of records. Then, shift the pointer to the right toolbar and select one of the several exporting methods: save it in multiple formats, download it as a PDF, email it, or save it to the cloud.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out patient reimbursement request form
How to fill out patient reimbursement request form
01
Obtain the patient reimbursement request form from your insurance provider or healthcare facility.
02
Fill in the patient's personal information, including name, address, date of birth, and contact details.
03
Provide details about the insurance policy, including the policy number and name of the insurance company.
04
Include information about the medical service rendered, such as the date of service, type of service, and the healthcare provider's information.
05
Attach all necessary documentation, including receipts, invoices, and any relevant medical records.
06
Review the completed form for accuracy and completeness.
07
Sign and date the form to certify that all information is true and complete.
08
Submit the form to the appropriate address or online portal as specified by the insurance provider.
Who needs patient reimbursement request form?
01
Patients who have incurred medical expenses and want reimbursement from their insurance provider.
02
Individuals who have received healthcare services and need to claim costs for covered services.
03
Caregivers or legal representatives acting on behalf of patients seeking reimbursement.
A comprehensive guide to the patient reimbursement request form
Understanding the patient reimbursement request form
The patient reimbursement request form is a vital document in the healthcare system designed to facilitate the process of requesting reimbursement for medical expenses incurred by patients. Its primary purpose is to provide healthcare payers, such as insurance companies, with essential information regarding expenses that should be covered under the patient's health plan.
This form is crucial because it streamlines the financial aspects of healthcare, ensuring patients are financially supported and can recover costs for services rendered, whether those services were provided at home, in the office, or during a telehealth session. By clearly outlining expenses, diagnosis codes, and procedure codes, the form simplifies the reimbursement process, making it easier for both patients and healthcare providers.
Facilitates timely reimbursements.
Provides clarity on covered medical services.
Standardizes the claim submission process.
Who needs to fill out this form?
Individuals seeking reimbursement must understand who the form is for. Primarily, patients who have paid for medical services out-of-pocket can fill out the patient reimbursement request form. However, healthcare providers can also submit this form on behalf of their patients, often aligning it with superbills that detail the services provided and their costs.
Moreover, insurance subscribers must fill out the form for their dependents, ensuring that all family members receive the necessary financial support for their healthcare expenses. This approach encourages families to manage their healthcare finances effectively, promoting timely submissions for reimbursement for services like office visits and medical equipment.
Patients who paid upfront for services.
Providers submitting on behalf of patients.
Insurance subscribers for dependents.
Components of the patient reimbursement request form
A well-structured patient reimbursement request form contains several essential components that ensure clarity and ease of understanding. The first part of the form gathers patient information, including the full name, contact details, and insurance information. Accurate patient data is crucial for processing reimbursement claims efficiently.
The second part includes provider information – such as the provider’s name and contact details. This ensures that the payer can reach the healthcare professional if more clarity is needed regarding the expenses submitted. Finally, payer information includes the insurance company name and policy number; all these elements facilitate the claim's assessment by the insurance provider.
Patient Information: Name, contact, and insurance details.
Provider Information: Name and contact details of the healthcare provider.
Payer Information: Insurance company name and policy number.
Detailed expense breakdown
One of the most critical sections of the patient reimbursement request form involves providing a detailed expense breakdown. This includes the date of service, the type of service or treatment received, and an itemized bill along with receipts for all expenses. This meticulous detailing is not only helpful for the payer but also essential for ensuring that the reimbursement amount aligns with the services rendered.
Additionally, if any discounts have been applied or payments made in advance, these should also be included to provide a comprehensive picture of the financial transaction related to healthcare services. By maintaining accuracy in this section, patients enhance their chances of a successful reimbursement process.
Date of Service: When the medical service was provided.
Type of Service: Describes the nature of the medical treatment or procedure.
Itemized Bill: Costs associated with each service or item.
Any Discounts: Noting any pre-paid amounts or discounts already applied.
Collecting required documentation
To ensure a smooth reimbursement process, collecting the required documentation is crucial. Key attachments include the Explanation of Benefits (EOB), which outlines how claims have been processed by the payer, and itemized bills from healthcare providers that detail the services rendered.
Organizing your documentation efficiently can prevent delays. Consider maintaining both digital copies for ease of access and physical copies for your records. Keep track of submission deadlines to ensure timely processing and avoid missing out on reimbursements that may become unattainable once deadlines pass.
Explanation of Benefits: Essential for understanding coverage.
Itemized Bills: Provide detailed accounts of services received.
Submission Deadlines: Important to note to ensure timely claims.
Steps to complete the patient reimbursement request form
Completing the patient reimbursement request form can be straightforward if done correctly. Start by following a clear step-by-step process, beginning with filling out personal information accurately. This includes ensuring correct spelling of your full name, contact information, and insurance details.
Next, move to the expense reporting section, where you will provide details about the services received and match them with the supporting documentation. When reporting expenses, be meticulous in noting service dates and the corresponding amounts billed. Taking the time to complete each section carefully is vital to avoid potential mistakes that could delay your reimbursement.
Fill out personal information: Ensure accuracy in all aspects.
Report expenses: Include all necessary details and match them with documentation.
Double-check for accuracy: Avoid common mistakes.
Finalizing your submission
Before submitting the patient reimbursement request form, take time to review every aspect of your submission. Checking for completeness and accuracy is essential in preventing issues later on. Ensure that you have included all required documentation attached to your claim, such as itemized bills and the necessary Explanation of Benefits.
When it comes to submission methods, you have options. Many payers allow for online submissions through their websites, which can expedite processing times. Alternatively, if mailing physical copies, keep a record of what you've sent and when. Tracking your submission can help you follow up effectively on the reimbursement status.
Review your submission thoroughly before sending.
Choose a submission method: online or physical.
Keep tracking records: Monitor the status of your submission.
What to expect after submission
After you've submitted your patient reimbursement request form, it's essential to understand the payer's review process. Generally, expect the reimbursement approval to take several weeks. During this time, the payer will evaluate the claim, confirming that all documentation meets their requirements.
In the event of a claim denial or delay, understanding your options becomes critical. You may need to directly contact the payer for clarification or consider appealing the decision. Staying informed about your submission status can make a difference in how quickly you receive any resolution.
Understand the review process: Know the typical timeframe.
Be prepared to handle denials or delays.
Contact the payer for further clarification when needed.
pdfFiller tools for managing your forms
Navigating the patient reimbursement request form can be made simpler with pdfFiller's tools. Its cloud-based platform enables you to seamlessly edit PDFs, eSign documents, and collaborate with others, making it an ideal solution for individuals and teams managing their healthcare forms.
Interactive tools for easy editing mean you can tailor your forms directly in the pdfFiller environment, addressing any special requirements specific to your situation. Also, with eSigning capabilities, you eliminate the delays often associated with physical signatures, facilitating faster processing of your reimbursement requests.
Interactive editing tools: Customize your forms easily.
eSigning capabilities: Speed up processing times.
Cloud-based access: Manage documents from anywhere.
Frequently asked questions (FAQs)
When dealing with the patient reimbursement request form, several common questions often arise. Patients frequently inquire about what specific information is necessary for a successful submission. Others may need clarification on the timeline for reimbursement or what actions to take in case of a denial.
Addressing these queries effectively helps to alleviate concerns and streamline the submission process. Be proactive in researching potential issues or requirements, ensuring you have a clear understanding of the process.
What information is required on the form?
How long does the reimbursement process take?
What should I do if my claim is denied?
Additional tools and resources available on pdfFiller
PdfFiller not only provides an efficient platform for the patient reimbursement request form but also offers a variety of related forms and resources that can be incredibly beneficial. Accessing interactive tutorials and guides can further enhance your understanding of how to navigate the intricacies of healthcare claims.
By leveraging these resources, you're able to improve your form-filling process, making the overall experience of managing your healthcare expenses more efficient and less stressful.
Related forms: Explore other healthcare-related documents.
Interactive tutorials: Get guidance on filling forms.
Comprehensive support: Access materials for various needs.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
Can I create an eSignature for the patient reimbursement request form in Gmail?
With pdfFiller's add-on, you may upload, type, or draw a signature in Gmail. You can eSign your patient reimbursement request form and other papers directly in your mailbox with pdfFiller. To preserve signed papers and your personal signatures, create an account.
How do I edit patient reimbursement request form on an iOS device?
Use the pdfFiller app for iOS to make, edit, and share patient reimbursement request form from your phone. Apple's store will have it up and running in no time. It's possible to get a free trial and choose a subscription plan that fits your needs.
How do I fill out patient reimbursement request form on an Android device?
On Android, use the pdfFiller mobile app to finish your patient reimbursement request form. Adding, editing, deleting text, signing, annotating, and more are all available with the app. All you need is a smartphone and internet.
What is patient reimbursement request form?
A patient reimbursement request form is a document used by patients to request reimbursement for medical expenses incurred due to healthcare services or treatments that were not covered by insurance.
Who is required to file patient reimbursement request form?
Patients who have incurred out-of-pocket medical expenses and wish to receive reimbursement from their insurance provider or other entities are required to file a patient reimbursement request form.
How to fill out patient reimbursement request form?
To fill out a patient reimbursement request form, one should gather the necessary medical bills, complete personal information, provide details of the services received, attach supporting documents such as receipts, and submit the form to the appropriate insurance provider.
What is the purpose of patient reimbursement request form?
The purpose of a patient reimbursement request form is to allow patients to seek compensation for medical expenses that they have paid out-of-pocket and to facilitate the claims process with insurance companies.
What information must be reported on patient reimbursement request form?
Information that must be reported on a patient reimbursement request form typically includes the patient's personal details, insurance information, a description of the services received, dates of service, amounts paid, and relevant documentation such as bills and receipts.
Fill out your patient reimbursement request form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Patient Reimbursement Request Form is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms




If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
