Medical Claim Form Template - Page 3



What is Medical Claim Form Template?
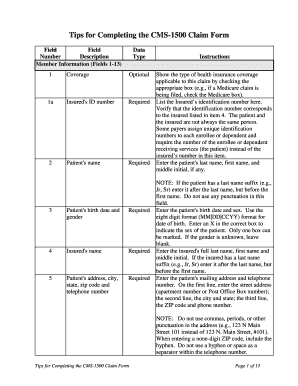
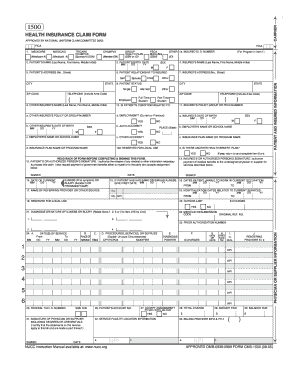
A Medical Claim Form Template is a standardized document used by healthcare providers to submit claims for reimbursement from insurance companies. It includes essential information such as patient details, treatment provided, and the cost of services.
What are the types of Medical Claim Form Template?
There are several types of Medical Claim Form Templates based on the type of insurance and the healthcare provider. Some common types include CMS-1500 for medical services, UB-04 for institutional providers, and ADA Dental Claim Form for dental services.
How to complete Medical Claim Form Template
Completing a Medical Claim Form Template is essential in ensuring timely reimbursement for healthcare services. Follow these steps to accurately fill out the form:
pdfFiller empowers users to create, edit, and share documents online. Offering unlimited fillable templates and powerful editing tools, pdfFiller is the only PDF editor users need to get their documents done.



