Family Medical History Form






What is Family Medical History Form?
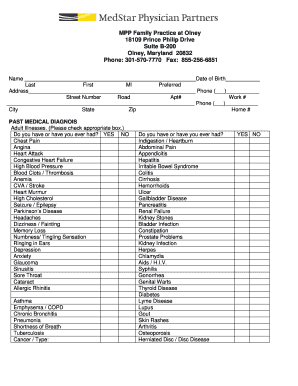
A Family Medical History Form is a document that records information about diseases and health conditions that run in a person's family. It helps healthcare providers understand the risk factors and genetic predispositions that may impact an individual's health.
What are the types of Family Medical History Form?
There are several types of Family Medical History Forms, including:
Basic Family Medical History Form
Comprehensive Family Medical History Form
Pediatric Family Medical History Form
Genetic Family Medical History Form
How to complete Family Medical History Form
Completing a Family Medical History Form is a simple process that involves the following steps:
01
Fill in your personal information, including name, date of birth, and contact details.
02
Provide details about your immediate family members' medical history, including parents, siblings, and children.
03
Include information about any significant health conditions or diseases that your family members have experienced.
04
Update the form regularly with any new health information or changes in your family's medical history.
05
Review and revise the form as needed before sharing it with your healthcare provider.
pdfFiller empowers users to create, edit, and share documents online. Offering unlimited fillable templates and powerful editing tools, pdfFiller is the only PDF editor users need to get their documents done.
Thousands of positive reviews can’t be wrong
Read more or give pdfFiller a try to experience the benefits for yourself