Get the free Patient Name Patient - Planned Parenthood - plannedparenthood
Show details
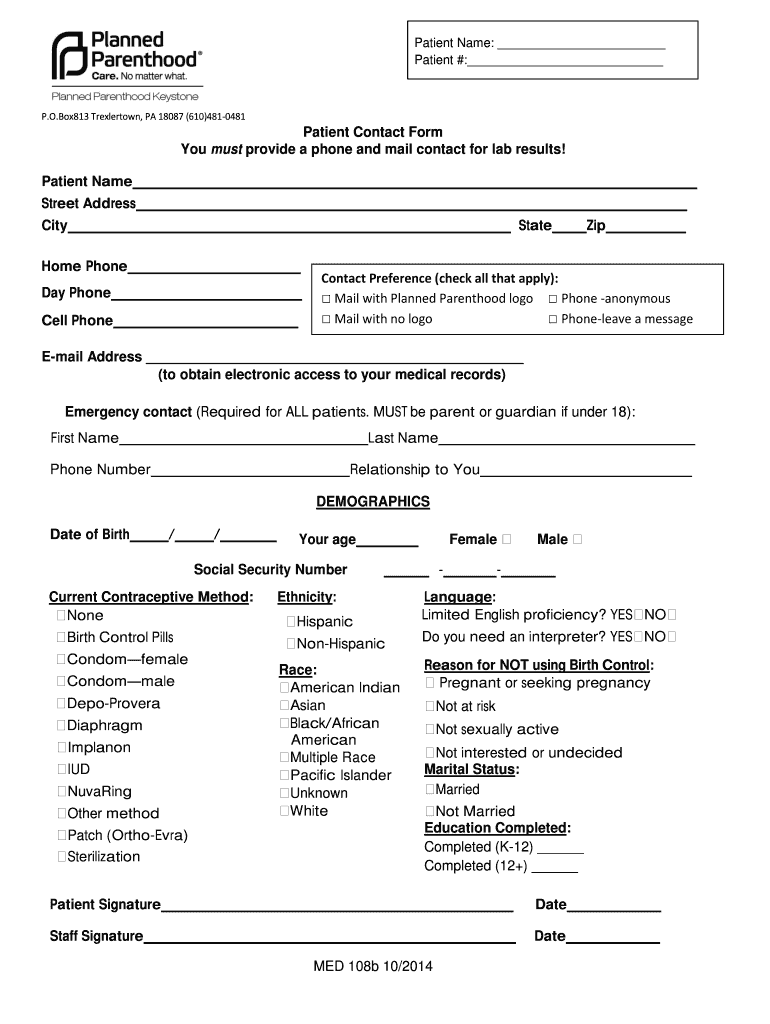
Patient Name: Patient #: P.O. Box813 Trexlertown, PA 18087 (610)4810481 Patient Contact Form You must provide a phone and mail contact for lab results! Patient Name Street Address City State Home
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign patient name patient
Edit your patient name patient form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your patient name patient form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit patient name patient online



Here are the steps you need to follow to get started with our professional PDF editor:
1
Create an account. Begin by choosing Start Free Trial and, if you are a new user, establish a profile.
2
Prepare a file. Use the Add New button. Then upload your file to the system from your device, importing it from internal mail, the cloud, or by adding its URL.
3
Edit patient name patient. Replace text, adding objects, rearranging pages, and more. Then select the Documents tab to combine, divide, lock or unlock the file.
4
Get your file. Select your file from the documents list and pick your export method. You may save it as a PDF, email it, or upload it to the cloud.
It's easier to work with documents with pdfFiller than you could have believed. You can sign up for an account to see for yourself.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out patient name patient
Question:
Write point by point how to fill out patient name patient. Who needs patient name patient?
Steps to fill out the patient name field:
01
Start by locating the patient name field on the form or electronic record.
02
Enter the patient's first name in the designated space.
03
Enter the patient's last name in the adjacent space.
04
Double-check the spelling of the patient's name for accuracy.
05
If the patient has a middle name or initial, enter it in the appropriate field, if available.
06
Ensure that the entered name reflects the patient's legal name and matches their identification documents, such as their driver's license or passport.
07
If the patient goes by a different name or has a preferred name, there may be an additional field for that information. Enter it accordingly.
08
After filling out the patient name section, proceed to complete the rest of the form or record as required.
Who needs patient name patient?
01
Healthcare providers: Healthcare professionals, including doctors, nurses, and other medical staff, require the patient name to obtain accurate identification and maintain proper medical records.
02
Medical billing and insurance departments: These departments need the patient's name to process insurance claims, create invoices, and ensure accurate reimbursement.
03
Pharmacies and laboratory facilities: Pharmacies and labs also require the patient's name to match prescriptions or test samples to the correct individual.
04
Medical researchers and statisticians: Professionals involved in medical research and data analysis rely on accurate patient names for recordkeeping and statistical analysis.
05
Government agencies: Health departments, regulatory bodies, and other government agencies may require patient names for public health monitoring and reporting purposes.
06
Legal and administrative purposes: Patient names may be necessary for legal or administrative reasons, such as consent forms, liability documentation, or patient privacy rights.
Note: The term "patient name patient" in the example may seem repetitive or erroneous. Please ensure to use the correct patient's name in practice.
Fill
form
: Try Risk Free
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
Where do I find patient name patient?
The premium version of pdfFiller gives you access to a huge library of fillable forms (more than 25 million fillable templates). You can download, fill out, print, and sign them all. State-specific patient name patient and other forms will be easy to find in the library. Find the template you need and use advanced editing tools to make it your own.
How do I fill out the patient name patient form on my smartphone?
Use the pdfFiller mobile app to fill out and sign patient name patient on your phone or tablet. Visit our website to learn more about our mobile apps, how they work, and how to get started.
How do I fill out patient name patient on an Android device?
Use the pdfFiller Android app to finish your patient name patient and other documents on your Android phone. The app has all the features you need to manage your documents, like editing content, eSigning, annotating, sharing files, and more. At any time, as long as there is an internet connection.
What is patient name patient?
Patient name patient is the name of the individual receiving medical treatment or services.
Who is required to file patient name patient?
Healthcare providers/organizations are required to file patient name patient.
How to fill out patient name patient?
Patient name patient should be filled out accurately and completely on medical records and billing forms.
What is the purpose of patient name patient?
The purpose of patient name patient is to identify the individual receiving medical treatment/services.
What information must be reported on patient name patient?
The patient name patient must include the full legal name of the individual.
Fill out your patient name patient online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Patient Name Patient is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms

If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
