
Health Partners CMS 1500 & UB04 2014-2025 free printable template
Show details
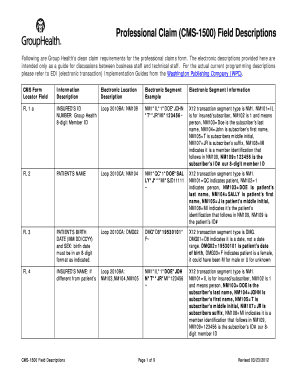
CMS 1500 and UB04 Claim Form
ANSI Mapping Guidelines for HIPAA v5010 (with errata)CMS 1500 Claim Form
When submitting claims on the CMS 1500 form, please use the following guidelines for
your paper
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign health cms1500 form hipaa

Edit your partners cms 1500 printable form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.

Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.

Share your form instantly
Email, fax, or share your cms1500 hipaa v5010 fillable form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit cms1500 hipaa v5010 online online



Follow the guidelines below to benefit from the PDF editor's expertise:
1
Register the account. Begin by clicking Start Free Trial and create a profile if you are a new user.
2
Simply add a document. Select Add New from your Dashboard and import a file into the system by uploading it from your device or importing it via the cloud, online, or internal mail. Then click Begin editing.
3
Edit health partners cms1500 v5010 form. Rearrange and rotate pages, insert new and alter existing texts, add new objects, and take advantage of other helpful tools. Click Done to apply changes and return to your Dashboard. Go to the Documents tab to access merging, splitting, locking, or unlocking functions.
4
Get your file. Select the name of your file in the docs list and choose your preferred exporting method. You can download it as a PDF, save it in another format, send it by email, or transfer it to the cloud.
It's easier to work with documents with pdfFiller than you could have believed. You can sign up for an account to see for yourself.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
Health Partners CMS 1500 & UB04 Form Versions
Version
Form Popularity
Fillable & printabley
How to fill out cms1500 mapping guidelines form

How to fill out Health Partners CMS 1500 & UB04
01
Obtain the CMS 1500 or UB04 forms from a reliable source.
02
Fill in the patient's personal information including name, address, and date of birth.
03
Provide the insurance information including the policy number and group number.
04
Enter the provider's information such as name, address, and NPI number.
05
Detail the services rendered, including dates of service, procedure codes, and diagnosis codes.
06
Include any necessary modifiers that apply to the procedure codes.
07
Calculate the total charges for the services provided.
08
Review the completed form for accuracy and completeness.
09
Submit the forms electronically or via mail to the appropriate payer.
Who needs Health Partners CMS 1500 & UB04?
01
Healthcare providers submitting claims for reimbursement from insurance companies.
02
Billing departments in medical facilities that process patient claims.
03
Medical practices and specialists providing services covered by health insurance.
04
Patients who are seeking reimbursement from their health insurance for medical services received.
Fill
form guideline
: Try Risk Free
People Also Ask about partners cms1500 guidelines v5010
What goes on a CMS 1500 form?
How to fill out a CMS-1500 form The type of insurance and the insured's ID number. The patient's full name. The patient's date of birth. The insured's full name, if applicable. The patient's address. The patient's relationship to the insured, if applicable. The insured's address, if applicable. Field reserved for NUCC use.
What is field 11 in CMS 1500 claim form?
KEY: R = Required | NR = Not Required | S = Situational, only use if appropriate specific to claim Field IDField DescriptionData Type10dCLAIM CODES (DESIGNATED BY NUCC)S11INSURED'S POLICY GROUP OR FECA NUMBERNR11aINSURED'S DATE OF BIRTH, GENDERNR11bOTHER CLAIM ID (DESIGNATED BY NUCC)NR59 more rows
What is field 9 in CMS 1500 claim form?
9. Name of the INSURED PERSON of other payer in Insurance Information screen under Patient Master.
What is the field 9 in CMS 1500 claim form?
9. Name of the INSURED PERSON of other payer in Insurance Information screen under Patient Master.
What is CMS 1500 form with description?
The CMS-1500 form is the standard claim form used by a non-institutional provider or supplier to bill Medicare carriers and durable medical equipment regional carriers (DMERCs) when a provider qualifies for a waiver from the Administrative Simplification Compliance Act (ASCA) requirement for electronic submission of
How do I submit a 1500 claim to Medicare?
CMS does not supply the form to providers for claim submission. In order to purchase claim forms, you should contact the U.S. Government Printing Office at 1-866-512-1800, local printing companies in your area, and/or office supply stores.
What will you enter in field 12 on the CMS 1500?
12. PATIENT'S OR AUTHORIZED PERSON'S SIGNATURE I authorize the release of any medical or other information necessary to process this claim. I also request payment of government benefits either to myself or to the party who accepts assignment below.
How to fill out diagnosis pointer on CMS 1500?
Enter the diagnosis reference number (pointer) in the unshaded area. The diagnosis pointer references the line number from field 21 that relates to the reason the service(s) was performed (ex. 1, 2, 3, or 4, or multiple numbers if the service relates to multiple diagnosis from field 21).
What is the field description of the CMS 1500 form?
Also known as the Healthcare Financing Administration (HCFA) form, the CMS-1500 form is used for claim reimbursement for several government insurance plans such as Medicaid, Tricare, and Medicare. In simple words, this form is used to bill for medical services provided to patients who are covered under insurance.
How to fill out a CMS 1500 form step by step?
How to fill out a CMS-1500 form The type of insurance and the insured's ID number. The patient's full name. The patient's date of birth. The insured's full name, if applicable. The patient's address. The patient's relationship to the insured, if applicable. The insured's address, if applicable. Field reserved for NUCC use.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
Can I create an eSignature for the cms1500 claim v5010 fillable in Gmail?
When you use pdfFiller's add-on for Gmail, you can add or type a signature. You can also draw a signature. pdfFiller lets you eSign your health cms1500 v5010 fillable and other documents right from your email. In order to keep signed documents and your own signatures, you need to sign up for an account.
How do I fill out the partners cms 1500 form form on my smartphone?
You can easily create and fill out legal forms with the help of the pdfFiller mobile app. Complete and sign cms1500 form mapping v5010 and other documents on your mobile device using the application. Visit pdfFiller’s webpage to learn more about the functionalities of the PDF editor.
How do I complete cms1500 mapping guidelines v5010 on an iOS device?
Download and install the pdfFiller iOS app. Then, launch the app and log in or create an account to have access to all of the editing tools of the solution. Upload your partners cms1500 guidelines form from your device or cloud storage to open it, or input the document URL. After filling out all of the essential areas in the document and eSigning it (if necessary), you may save it or share it with others.
What is Health Partners CMS 1500 & UB04?
Health Partners CMS 1500 is a standardized form used primarily by healthcare providers to bill for outpatient services, while UB04 is used for inpatient hospital services. Both forms facilitate the submission of claims for reimbursement from insurance providers.
Who is required to file Health Partners CMS 1500 & UB04?
Healthcare providers, including physicians, outpatient facilities, and hospitals, are required to file Health Partners CMS 1500 for outpatient services and UB04 for inpatient services to ensure proper billing and reimbursement from insurance programs.
How to fill out Health Partners CMS 1500 & UB04?
To fill out Health Partners CMS 1500, providers must enter patient and insurance information, diagnosis codes, procedure codes, and billing information accurately in the designated fields. For UB04, providers must include details about the hospital stay, including admission and discharge dates, patient information, diagnosis, and services provided. It's important to follow specific guidelines and instructions for each form to avoid claim denials.
What is the purpose of Health Partners CMS 1500 & UB04?
The purpose of Health Partners CMS 1500 & UB04 is to provide a standardized means of submitting claims for healthcare services rendered to patients to facilitate payment by health insurance companies and government payers.
What information must be reported on Health Partners CMS 1500 & UB04?
Health Partners CMS 1500 requires information such as patient demographics, insurance details, diagnosis codes (ICD), and procedure codes (CPT/HCPCS). UB04 must report similar information but in a different format, including patient demographics, admission dates, discharge dates, diagnosis codes, revenue codes, and service details.
Fill out your cms1500 claim v5010 2014-2025 online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
cms1500 Claim Mapping Guidelines is not the form you're looking for?Search for another form here.
Keywords relevant to cms1500 mapping guidelines hipaa
Related to cms1500 ansi hipaa v5010







If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
