WellCare Provider Appeal Request Form 2010-2024 free printable template
Show details
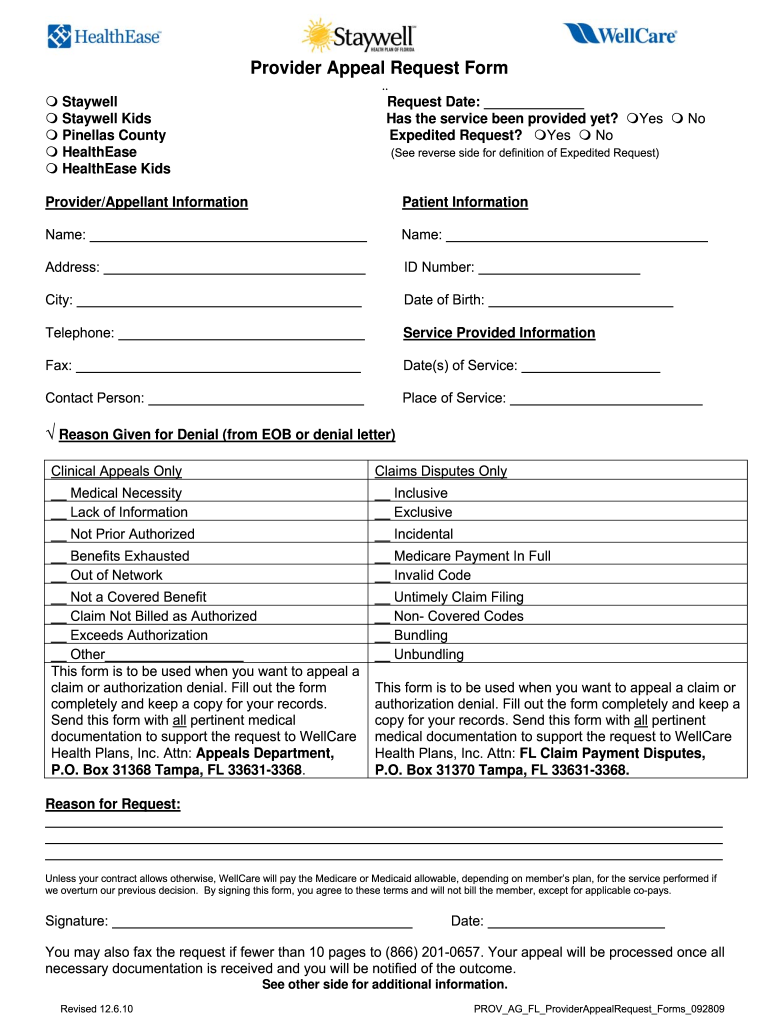
Provider Appeal Request Form. Request Date Has the service been provided yet Expedited Request Yes No Staywell Staywell Kids Pinellas County HealthEase See reverse side for definition of Expedited Request Patient Information Name Address ID Number City Date of Birth Telephone Service Provided Information Fax Date s of Service Contact Person Place of Service Reason Given for Denial from EOB or denial letter Clinical Appeals Only Claims Disputes O...
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign

Edit your wellcare appeal form form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.

Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.

Share your form instantly
Email, fax, or share your wellcare appeal form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit wellcare appeal form online



Follow the steps down below to take advantage of the professional PDF editor:
1
Check your account. It's time to start your free trial.
2
Simply add a document. Select Add New from your Dashboard and import a file into the system by uploading it from your device or importing it via the cloud, online, or internal mail. Then click Begin editing.
3
Edit wellcare appeal form pdf. Rearrange and rotate pages, insert new and alter existing texts, add new objects, and take advantage of other helpful tools. Click Done to apply changes and return to your Dashboard. Go to the Documents tab to access merging, splitting, locking, or unlocking functions.
4
Save your file. Select it from your records list. Then, click the right toolbar and select one of the various exporting options: save in numerous formats, download as PDF, email, or cloud.
pdfFiller makes dealing with documents a breeze. Create an account to find out!
How to fill out wellcare appeal form

How to fill out wellcare appeal form pdf?
01
Gather all necessary information and documentation to support your appeal, such as medical records, letters from healthcare providers, and any other relevant documents.
02
Open the wellcare appeal form pdf on your computer or device.
03
Carefully read and understand the instructions provided on the form. Make sure to follow them accurately.
04
Begin filling out the form by entering your personal information, including your name, address, phone number, and wellcare identification number.
05
Provide a detailed description of the reason for your appeal. Clearly explain why you believe the initial decision was incorrect or unfair.
06
Use the space provided to attach and reference any supporting documentation that you have gathered. Make sure to clearly label each document and refer to it in your written explanation.
07
Review the completed form to ensure that all information is accurate and all required sections have been filled out.
08
Print the completed form and sign it according to the instructions provided.
09
Make a copy of the filled-out form and all attached documentation for your records.
10
Submit the appeal form and any supporting documents to wellcare according to their specified submission process.
Who needs wellcare appeal form pdf?
01
Individuals who have received an unfavorable decision or denial from wellcare regarding their healthcare coverage or benefits.
02
Those who believe that wellcare has made an incorrect determination and wish to challenge that decision.
03
Patients who require a formal appeal process with wellcare in order to seek a review and potential reversal of their initial decision.
Fill wellcare appeal form online : Try Risk Free
Our user reviews speak for themselves
Read more or give pdfFiller a try to experience the benefits for yourself
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
What is wellcare appeal form pdf?
Wellcare Appeal Form PDF is a document that individuals can use to file an appeal against a decision made by Wellcare Health Plans, Inc. This form is used to initiate a review of the decision and provide supporting documentation to demonstrate why the decision should be overturned. The form can be found on the Wellcare website or downloaded from the link provided.
Who is required to file wellcare appeal form pdf?
Anyone who is filing an appeal with WellCare for a denied request must submit the WellCare Appeal Form PDF. This form must be completed and signed by the member or the member's representative and can be found on the WellCare website.
What is the purpose of wellcare appeal form pdf?
The WellCare Appeal Form is used to submit an appeal when an individual or provider has disagreed with a decision made by WellCare, such as a denial of a request for coverage of a service or medication. The form provides a place for the individual or provider to outline the basis for their appeal and provide any additional information that may be needed. The form also provides a place for WellCare to respond to the appeal.
How to fill out wellcare appeal form pdf?
To fill out the WellCare appeal form PDF, follow the steps below:
1. Open the PDF form with a PDF reader software such as Adobe Acrobat Reader.
2. Click on the fields within the form to activate the text boxes where you need to enter information.
3. Start with the first section, which usually asks for your personal details such as your name, address, phone number, date of birth, and member ID number. Fill in this information accurately.
4. Move on to the next section, where you will have to provide the details of the appeal itself. This may include a description of the reason for the appeal, the date the original decision was made, the type of coverage or service being appealed, and any supporting documentation you may have. Fill in this information as accurately and completely as possible.
5. Some forms may also have sections where you need to select checkboxes or circle options to indicate certain conditions or choices. Make sure to read and understand the options before making your selection.
6. If there are any additional sections or fields specifically related to your appeal, fill them out accordingly.
7. Review the completed form carefully to ensure all the information you provided is accurate and legible.
8. If required, sign and date the form at the designated section. Some PDF readers offer options for electronic signatures, or you may need to print the form, sign it with a pen, and then scan it back to a digital format.
9. Save a copy of the completed form for your records, and also consider printing a physical copy if needed.
10. Submit the form according to the instructions provided on the form. This may include mailing it to the appropriate address or submitting it online through a specific portal.
Remember to consult the specific instructions provided with the appeal form, as requirements may vary depending on the organization or insurance provider.
What information must be reported on wellcare appeal form pdf?
The information that must be reported on a WellCare appeal form PDF includes:
1. Member Information: This includes the member's full name, WellCare member ID number, date of birth, contact information, and the member's relationship to the person filing the appeal (if applicable).
2. Provider Information: If the appeal is being filed by a healthcare provider on behalf of the member, their name, address, contact information, and National Provider Identifier (NPI) should be provided.
3. Reason for Appeal: A clear explanation of why the appeal is being filed, including details about the specific issue or denial that is being appealed. This could include denial of coverage for a specific treatment or medication, denial of a claim, or any other matter being disputed.
4. Supporting Documentation: Any relevant documentation that supports the appeal should be attached to the form. This may include medical records, test results, letters from healthcare providers, or any other documentation that helps provide evidence for the appeal.
5. Desired Outcome: The form should clearly state the desired outcome or resolution requested by the person filing the appeal. This could be a request to reconsider a denial, approve coverage for a treatment or medication, or any other specific outcome the person is seeking.
6. Signature: The form should be signed and dated by the person filing the appeal or their authorized representative, acknowledging that the information provided is accurate to the best of their knowledge.
Note: The specific information required on a WellCare appeal form PDF may vary depending on the specific circumstances and the type of appeal being filed. It is recommended to refer to the official WellCare appeal form or contact WellCare directly for the most accurate and up-to-date information.
How do I complete wellcare appeal form online?
Filling out and eSigning wellcare appeal form pdf is now simple. The solution allows you to change and reorganize PDF text, add fillable fields, and eSign the document. Start a free trial of pdfFiller, the best document editing solution.
How do I edit wellcare provider appeal form pdf online?
The editing procedure is simple with pdfFiller. Open your wellcare medicare appeal form in the editor. You may also add photos, draw arrows and lines, insert sticky notes and text boxes, and more.
How can I fill out wellcare provider appeal form on an iOS device?
Download and install the pdfFiller iOS app. Then, launch the app and log in or create an account to have access to all of the editing tools of the solution. Upload your wellcare appeal form 2023 from your device or cloud storage to open it, or input the document URL. After filling out all of the essential areas in the document and eSigning it (if necessary), you may save it or share it with others.
Fill out your wellcare appeal form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Wellcare Provider Appeal Form Pdf is not the form you're looking for?Search for another form here.
Keywords relevant to wellcare appeal form editable
Related to wellcare payment dispute form






If you believe that this page should be taken down, please follow our DMCA take down process
here
.
