Last updated on Mar 31, 2026
Amerigroup Pharmacy Prior Authorization Form free printable template
pdfFiller is not affiliated with any government organization

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
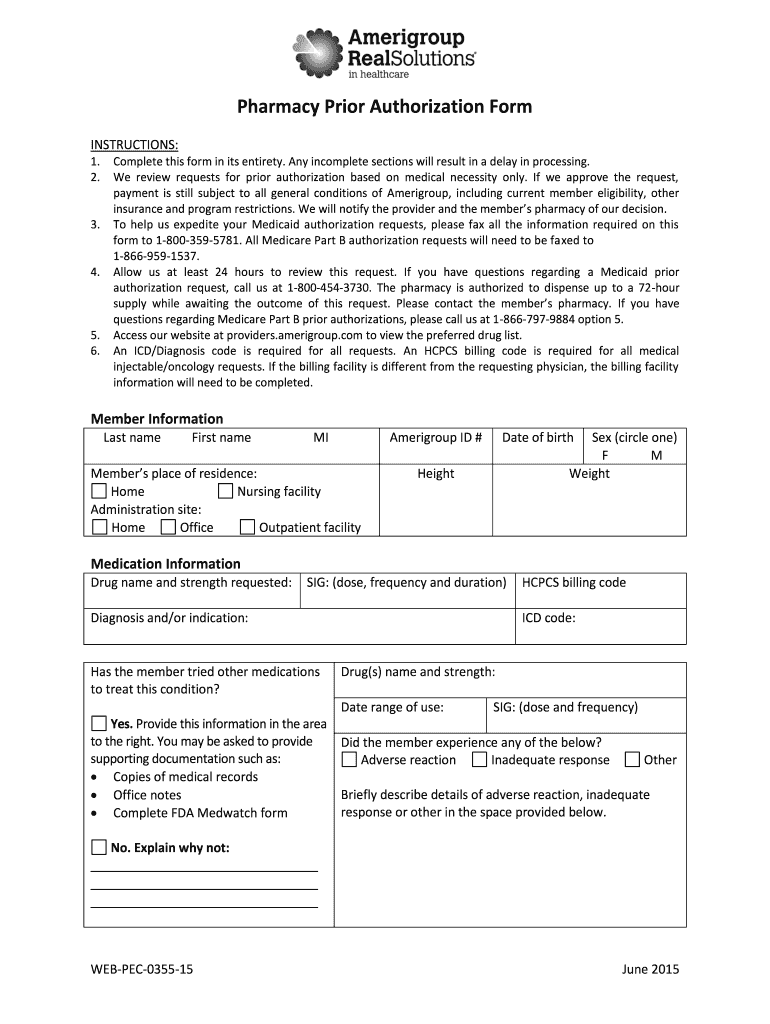
What is Amerigroup Pharmacy Prior Authorization Form
The Pharmacy Prior Authorization Form is a healthcare document used by prescribers to request approval from Amerigroup for medication coverage under Medicaid or Medicare Part B.
pdfFiller scores top ratings on review platforms
Who needs Amerigroup Pharmacy Prior Authorization Form?
Explore how professionals across industries use pdfFiller.

Amerigroup Pharmacy Prior Authorization Form is needed by:
-
Healthcare providers seeking medication approval
-
Pharmacists dispensing medications under prior authorization
-
Insurance agents assisting with patient coverage inquiries
-
Patients requiring authorization for medication costs
-
Medical offices managing patient care and prescriptions
-
Prescribers ensuring medication compliance with insurance
-
Billing departments handling prior authorization processes
Comprehensive Guide to Amerigroup Pharmacy Prior Authorization Form
What is the Pharmacy Prior Authorization Form?
The Pharmacy Prior Authorization Form is a critical document used by healthcare providers to obtain necessary approval for medication coverage under Medicaid and Medicare Part B. This form helps ensure that patients receive the medications prescribed by their healthcare professionals while adhering to regulatory requirements.
Healthcare providers, specifically prescribers, are required to complete and sign this form to initiate the prior authorization process. Its significance in the healthcare system cannot be understated, as it plays a vital role in improving patient access to medication and aligning treatment with insurance coverage policies.
Understanding the importance of the Pharmacy Prior Authorization Form benefits both patients and providers by facilitating the necessary communication with Medicare and Medicaid programs, ensuring comprehensive healthcare coverage.
Purpose and Benefits of the Pharmacy Prior Authorization Form
The primary purpose of the Pharmacy Prior Authorization Form is to streamline the approval process for medication coverage, significantly benefiting both healthcare providers and patients. By obtaining prior authorization, healthcare providers can ensure that medications are covered, thereby reducing potential out-of-pocket expenses for patients.
Additionally, this form can improve patient health outcomes by expediting access to necessary medications. When prior authorization is successfully obtained, it minimizes treatment delays, enabling patients to receive their prescribed therapies in a timely manner.
Ultimately, utilizing the Pharmacy Prior Authorization Form enhances the overall efficiency of the authorization process, specifically with providers like Amerigroup, leading to improved patient satisfaction and adherence to treatment protocols.
Who Needs the Pharmacy Prior Authorization Form?
Several key stakeholders require the Pharmacy Prior Authorization Form to ensure medication coverage is obtained efficiently. First and foremost, healthcare providers, particularly prescribers, must complete this form to initiate the authorization process.
Patients who are insured under Medicaid or Medicare Part B are also crucially impacted by this form, as their required medications must often go through an approval process before being dispensed. Furthermore, pharmacies play an essential role in facilitating the authorization request by submitting the completed form to the appropriate channels.
In essence, the Pharmacy Prior Authorization Form serves as an important tool for healthcare providers, patients, and pharmacies alike, ensuring that medication coverage is accessible and compliant with relevant healthcare guidelines.
How to Fill Out the Pharmacy Prior Authorization Form Online
Filling out the Pharmacy Prior Authorization Form online can be done efficiently through a platform like pdfFiller. Here’s a step-by-step guide for completing the form:
-
Access the online form through pdfFiller.
-
Begin by entering member details, including name, date of birth, and insurance information.
-
Provide specific medication details, including dosage and quantity required.
-
Complete the prescriber information section, ensuring accurate contact details are included.
-
Review all entered information for accuracy and completeness.
-
Sign digitally to authenticate the form, ensuring all required fields are filled out properly.
Understanding the key sections and instructions simplifies the process, allowing for an optimal experience in filling out essential fields and completing checkboxes as required.
Common Errors in Submitting the Pharmacy Prior Authorization Form
Submitting the Pharmacy Prior Authorization Form requires attention to detail to avoid common mistakes that could result in delays or rejections. Here’s a list of frequent errors to watch for:
-
Missing required signatures from the prescriber.
-
Inaccurate member or medication information.
-
Inadequate documentation or supporting materials accompanying the submission.
To prevent these issues, it is essential to utilize a review checklist before submission, ensuring all details are accurate and complete. Additionally, verifying that all necessary supporting documents are included will increase the likelihood of successful authorization.
How to Submit the Pharmacy Prior Authorization Form
Once the Pharmacy Prior Authorization Form is completed, submitting it correctly is crucial for timely processing. There are several methods to submit the completed form:
-
Fax the form to the designated number provided by the insurance company.
-
Utilize online submission options available through the healthcare provider's system.
Be mindful of submission timelines and processing times to ensure the request is handled promptly. Tracking your submission can provide reassurance and help manage expectations regarding the follow-up process with the insurance provider.
What Happens After You Submit the Form?
After submitting the Pharmacy Prior Authorization Form, it will undergo a review process by Amerigroup or other relevant insurers. Typically, you can expect a decision within a specific timeframe, which can vary based on the complexity of the request.
During this review period, you have the ability to check the status of your application, allowing you to remain informed about its progress. If a request is denied, knowing the steps to take for an appeal is critical, including gathering additional documentation to support your case.
Security and Compliance when Filling Out the Pharmacy Prior Authorization Form
When handling sensitive medical documents such as the Pharmacy Prior Authorization Form, security and compliance are of utmost importance. pdfFiller employs robust data protection measures, including encryption, to safeguard the information provided.
Furthermore, compliance with HIPAA and GDPR regulations ensures that the confidentiality of medical information shared during the authorization process is maintained. Users are advised to manage document retention securely to uphold the integrity of the information exchanged.
Enhance Your Experience with pdfFiller
Utilizing pdfFiller for filling out the Pharmacy Prior Authorization Form enhances the overall experience through its range of features. The platform allows users to eSign, edit documents, and access cloud storage, making it easier to retain completed forms for future reference.
The user-friendly interface of pdfFiller simplifies the form-filling process for healthcare documentation, ensuring that users can efficiently manage their healthcare documents with confidence.
Sample or Example of a Completed Pharmacy Prior Authorization Form
Providing users with a visual example of a fully completed Pharmacy Prior Authorization Form can serve as an invaluable reference. This sample illustrates each section of the form filled out correctly, demonstrating alignment with required instructions.
Users are encouraged to utilize this example to ensure accuracy in their own submissions, comparing filled sections to confirm they have met all requirements before finalizing their forms.
How to fill out the Amerigroup Pharmacy Prior Authorization Form
-
1.Access pdfFiller and search for the 'Pharmacy Prior Authorization Form' using the search bar.
-
2.Open the document to view the fillable fields clearly displayed within the interface.
-
3.Before starting, gather all necessary information such as member details, medication, diagnosis, and prescriber information.
-
4.Begin by entering the member's personal information into the designated fields at the top of the form.
-
5.Continue on to provide the medication details, ensuring accurate dosages and medication names are input correctly.
-
6.Fill in the diagnosis section with relevant medical information regarding the patient's health condition.
-
7.Utilize pdfFiller's checkboxes to indicate any additional qualifications or reasons for the prior authorization request.
-
8.Review the completed form systematically to ensure all fields are appropriately filled and there are no missed sections.
-
9.Make sure to sign the form in the designated signature line to confirm completion and authorization.
-
10.Attach any required supporting documentation directly within pdfFiller using the upload feature.
-
11.Once all details are correct and documents are attached, save the form securely within your pdfFiller account.
-
12.Finally, submit the form by clicking the 'Send' button and selecting the appropriate fax option for submission to Amerigroup.

Who is eligible to use the Pharmacy Prior Authorization Form?
Healthcare providers and prescribers are eligible to use this form to request medication coverage for patients under Medicaid and Medicare Part B. Ensure that the requests are in compliance with relevant regulations.
What documents are needed to complete this form?
You will need to provide the member's personal information, medication details, diagnosis, and prescriber credentials. Supporting documentation may also be required for the authorization request.
How do I submit the completed form?
After filling out the Pharmacy Prior Authorization Form on pdfFiller, you can submit it by selecting the fax option to send it directly to Amerigroup or download it for manual submission.
Are there deadlines for submitting the prior authorization request?
There are usually time-sensitive aspects of prior authorization requests. It’s essential to submit the form as soon as the need arises to avoid delays in medication dispensing.
What are common mistakes to avoid when completing the form?
Common mistakes include missing signatures, incomplete information, and not attaching required documentation. Double-checking each section before submitting helps avoid these errors.
What is the processing time for prior authorization requests?
Processing times for prior authorization requests can vary. Typically, expect a response within a few business days, but urgent requests might have expedited processing.
Can patients fill out and submit this form directly?
No, this form must be completed and signed by the prescriber. Patients should work with their healthcare providers to ensure the form is filled out correctly.
Amerigroup Pharmacy Prior Authorization Form Form Versions
Related Content
Related Forms




Related Catalogs

If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.