Generic Authorization To Release Medical Records Form


What is Generic Authorization To Release Medical Records Form?
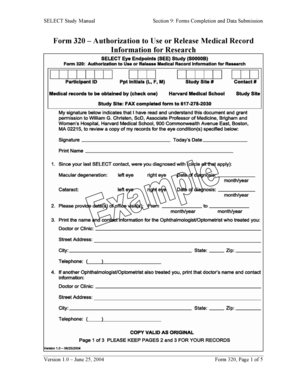
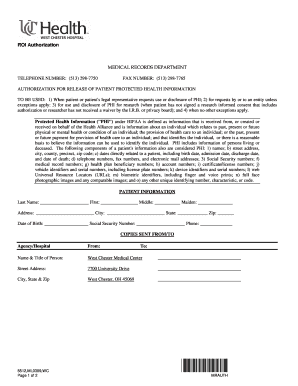
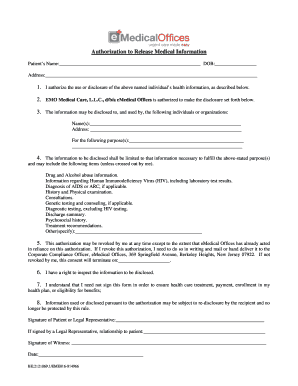
The Generic Authorization To Release Medical Records Form is a legal document that grants permission to healthcare providers to release a patient's medical records to a third party. This form ensures that the patient's confidentiality and privacy rights are protected while allowing the sharing of necessary medical information.
What are the types of Generic Authorization To Release Medical Records Form?
There are several types of Generic Authorization To Release Medical Records Forms that cater to different situations. Some common types include: 1. Standard Generic Authorization Form: This form is used for general requests to release medical records. 2. Specific Purpose Authorization Form: This form is used when the release of medical records is limited to a specific purpose or recipient. 3. Limited Time Authorization Form: This form grants authorization to release medical records for a specified period of time. 4. Mental Health Authorization Form: This form is specifically designed for the release of mental health-related records.
How to complete Generic Authorization To Release Medical Records Form
Completing a Generic Authorization To Release Medical Records Form is a straightforward process. Here are the basic steps to follow: 1. Obtain the Form: Download or request a copy of the form from the healthcare provider or hospital where the medical records are held. 2. Provide Patient Information: Fill in the patient's personal information, such as name, date of birth, and contact details. 3. Specify Purpose and Recipient: Clearly state the purpose for releasing the medical records and the recipient's information. 4. Include Relevant Dates: Specify the timeframe or dates during which the authorization is valid, if applicable. 5. Sign and Date: The patient or legal guardian must sign and date the form to make it legally binding. 6. Submit the Form: Send the completed form to the healthcare provider or hospital as instructed.
pdfFiller empowers users to create, edit, and share documents online. Offering unlimited fillable templates and powerful editing tools, pdfFiller is the only PDF editor users need to get their documents done.