Fmla Eligibility Form









What is Fmla Eligibility Form?
The FMLA Eligibility Form, also known as the Family and Medical Leave Act Eligibility Form, is a document that employees can use to determine if they qualify for leave under the FMLA. This form helps employees understand their rights and responsibilities when taking FMLA leave.
What are the types of Fmla Eligibility Form?
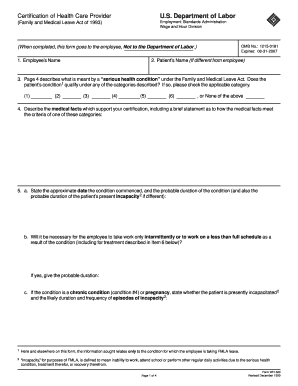
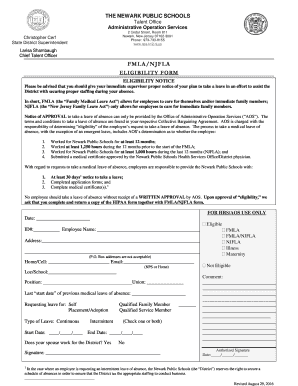
There are several types of FMLA Eligibility Forms that employees may encounter. Some common types include: 1. FMLA Employee Eligibility Form 2. FMLA Certification of Health Care Provider Form 3. FMLA Designation Notice Form 4. FMLA Recertification Form 5. FMLA Military Family Leave Eligibility Form
How to complete Fmla Eligibility Form
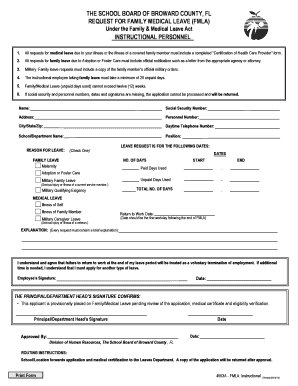
Completing the FMLA Eligibility Form is a straightforward process. Here are the steps to successfully fill out the form: 1. Obtain the FMLA Eligibility Form from your employer or human resources department. 2. Fill in your personal information, including your name, employee ID, and contact information. 3. Provide details about your medical condition or family member's medical condition that necessitates FMLA leave. 4. Have your healthcare provider complete the relevant sections of the form if required. 5. Submit the completed form to your employer for review and approval.
pdfFiller empowers users to create, edit, and share documents online. Offering unlimited fillable templates and powerful editing tools, pdfFiller is the only PDF editor users need to get their documents done.