Medical Claim Form





What is a Medical Claim Form?
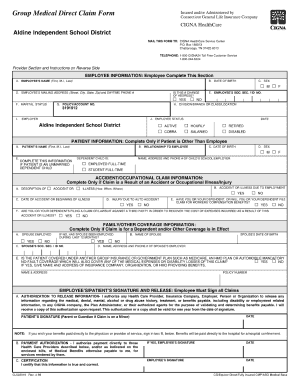
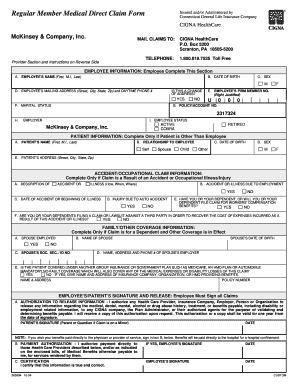
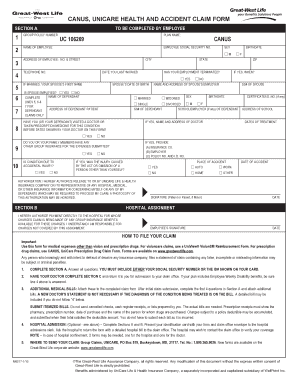
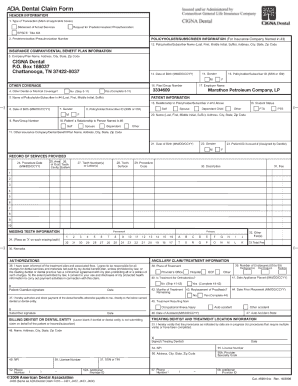
A Medical Claim Form is a document used to request reimbursement for healthcare services provided by a healthcare provider. It typically includes information such as patient details, the services provided, costs incurred, and any insurance information.
What are the types of Medical Claim Form?
There are several types of Medical Claim Forms, including:
CMS-1500 Form: Used for billing individual healthcare services provided by physicians or healthcare professionals.
UB-04 Form: Used for inpatient and outpatient hospital claims.
ADA Dental Claim Form: Specifically for dental services and treatments.
How to complete Medical Claim Form
Completing a Medical Claim Form can seem confusing at first, but with the right guidance, it can be straightforward. Here are some steps to help you complete the form:
01
Gather all necessary documents, including bills, insurance information, and receipts.
02
Fill in your personal information accurately, including your name, address, and insurance policy number.
03
Provide details of the healthcare services received, including dates, procedures, and costs.
04
Double-check all information for accuracy before submitting the form.
pdfFiller empowers users to create, edit, and share documents online. Offering unlimited fillable templates and powerful editing tools, pdfFiller is the only PDF editor users need to get their documents done.
Thousands of positive reviews can’t be wrong
Read more or give pdfFiller a try to experience the benefits for yourself
Related templates