1500 Claim Form Example





What is 1500 Claim Form Example?
The 1500 Claim Form Example is a standard form used by healthcare providers to bill insurance companies for services provided to patients.
What are the types of 1500 Claim Form Example?
There are different types of 1500 Claim Form Examples based on the type of insurance claim being filed. Some common types include:
Professional Claims
Institutional Claims
Dental Claims
How to complete 1500 Claim Form Example
Completing the 1500 Claim Form Example is simple and straightforward. Follow these steps to ensure accuracy:
01
Fill in patient information accurately
02
Include provider details
03
Document service provided and charges
04
Submit the form to the insurance company for processing
pdfFiller empowers users to create, edit, and share documents online. Offering unlimited fillable templates and powerful editing tools, pdfFiller is the only PDF editor users need to get their documents done.
Video Tutorial How to Fill Out 1500 Claim Form Example
Thousands of positive reviews can’t be wrong
Read more or give pdfFiller a try to experience the benefits for yourself
Questions & answers
Can you handwrite on a 1500 claim form?
Submission of the CMS 1500 (02/12) claim form should either be typed or computer printed forms. Handwritten forms can cause delays and errors in processing and slow down time for reimbursement. Ensure to use all capital typeface with Courier New or Tines New Roman font style and size 10.
How do I fill out a 1500 claim form?
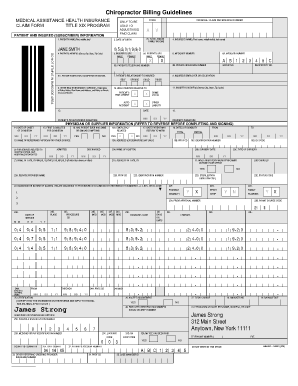
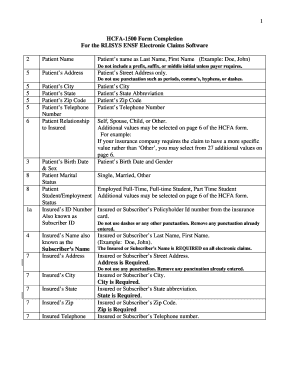
How to fill out a CMS-1500 form The type of insurance and the insured's ID number. The patient's full name. The patient's date of birth. The insured's full name, if applicable. The patient's address. The patient's relationship to the insured, if applicable. The insured's address, if applicable. Field reserved for NUCC use.
What is the resubmission code on Form 1500?
Professional Claims If you are submitting a void/replacement paper CMS 1500 claim, please complete box 22. For replacement or corrected claim enter resubmission code 7 in the left side of item 22 and enter the original claim number of the claim you are replacing in the right side of item 22.
Where is the taxonomy code on a 1500 claim form?
On a CMS-1500 paper claim, the taxonomy code is entered utilizing two fields on the claim form: Field 24I (upper shaded portion) = ID Qualifier: enter "ZZ" Field 24J (upper shaded portion) = rendering provider taxonomy code: enter the 10-digit taxonomy code.
What codes are used on a 1500 claim form?
Other CMS-1500 Codes Box 11b - Other Claim ID. Box 14 - Date of Current Illness, Injury, or Pregnancy (LMP) Box 15 - Other Date. Box 17 - Name of Referring Provider or Other Source. Box 17a, 19, 24i, 32b, 33b - Identifier Qualifiers. Box 21 - ICD indicator. Box 22 - Bill Frequency Code. Box 24h - EPSDT Reason Codes.
What are the codes used to report procedures on CMS 1500 claim forms called?
ICD-10-CM codes are reported on UB-04 claims and CMS 1500 claims.
Related templates