Free Medical Release Form Texas





What is Free Medical Release Form Texas?
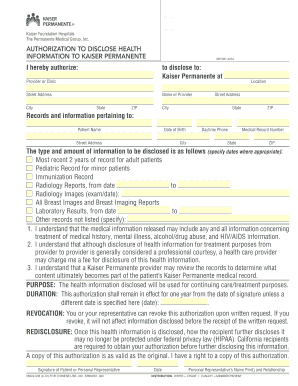
A Free Medical Release Form Texas is a legal document that allows an individual to authorize the release of their medical information to a specified party, such as a healthcare provider, insurance company, or legal representative. This form is essential for ensuring proper and timely access to medical records when needed.
What are the types of Free Medical Release Form Texas?
There are several types of Free Medical Release Form Texas, including but not limited to:
Standard Medical Release Form
HIPAA Release Form
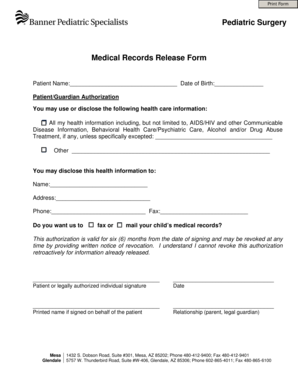
Minor Medical Release Form
How to complete Free Medical Release Form Texas
Completing a Free Medical Release Form Texas is a straightforward process that involves the following steps:
01
Gather personal information including name, date of birth, and contact information
02
Specify the party or parties authorized to receive the medical information
03
Sign and date the form in the presence of a witness, if required
04
Submit the completed form to the designated recipient
pdfFiller empowers users to create, edit, and share documents online. Offering unlimited fillable templates and powerful editing tools, pdfFiller is the only PDF editor users need to get their documents done.
Video Tutorial How to Fill Out Free Medical Release Form Texas
Thousands of positive reviews can’t be wrong
Read more or give pdfFiller a try to experience the benefits for yourself
Questions & answers
What is required for a HIPAA release?
The core elements of a valid authorization include: A meaningful description of the information to be disclosed. The name of the individual or the name of the person authorized to make the requested disclosure. The name or other identification of the recipient of the information.
How long does a doctor have to release medical records in Texas?
(b) Deadline for Release of Records. The requested copies of medical and/or billing records or a summary or narrative of the records shall be furnished by the physician within 15 business days after the date of receipt of the request and reasonable fees for furnishing the information.
What document must be signed to release medical information?
The Health Insurance Portability and Accountability Act of 1996 was put in place to help ensure privacy and yet ease of access to your medical records. A HIPAA Authorization Form is a document that allows a medical provider to share specific health information with another person or group.
How to fill out authorization for release of protected health information?
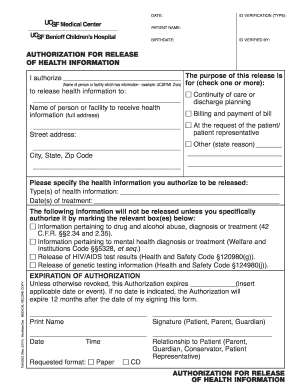
The complete name of the person or entity to receive the protected health information (PHI) A specific description of the information to be used or disclosed, including the dates of service. The purpose of the requested use and disclosure.
What document must be signed to release medical information Chapter 8?
The authorization form must give the patient the opportunity to limit the information to be released.
What must be included on a release of information form in a medical practice?
Elements of a release form Patient information. Naturally, the release should require the patient's information so it's clear who the form refers to. Receiving party's information. Information to be shared. Purpose of the release. Expiration of authorization. Disclaimers. Date and signature.
Related templates