Last updated on May 4, 2026
ECMC LGL 100 2013 free printable template
pdfFiller is not affiliated with any government organization

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is ECMC LGL 100
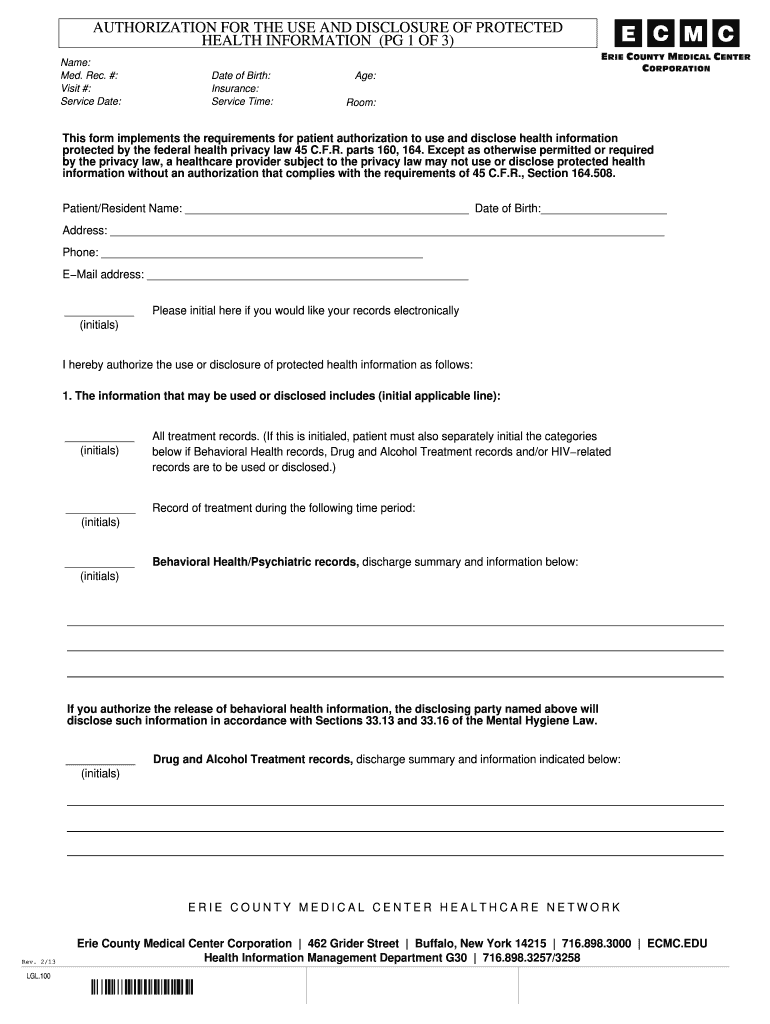
The Authorization for Use and Disclosure of Protected Health Information is a medical consent form used by patients to authorize the release of their health information.
pdfFiller scores top ratings on review platforms
Who needs ECMC LGL 100?
Explore how professionals across industries use pdfFiller.

ECMC LGL 100 is needed by:
-
Patients seeking to release their health records
-
Healthcare providers needing permission to disclose information
-
Personal representatives authorized to act on a patient's behalf
-
Healthcare facilities requiring documentation for compliance
-
Legal representatives involved in healthcare disputes
Comprehensive Guide to ECMC LGL 100
What is the Authorization for Use and Disclosure of Protected Health Information?
The Authorization for Use and Disclosure of Protected Health Information is a critical document that allows patients to permit healthcare providers to share their medical records. In accordance with HIPAA regulations, this form safeguards the privacy of individuals' health information while ensuring that essential data can be accessed when required. It typically includes key components such as patient information and specifies the types of records authorized for sharing.
Purpose and Benefits of the Authorization for Use and Disclosure of Protected Health Information
This authorization form is essential as it provides numerous benefits for both patients and healthcare providers. It facilitates the secure and efficient sharing of important health data, which can be crucial for ongoing treatment and care. Completing this form also has legal implications; if not filled out correctly, healthcare entities may face challenges in accessing necessary patient information.
Who Needs to Complete the Authorization for Use and Disclosure of Protected Health Information?
The target audience for this form includes patients seeking to control the flow of their medical information, as well as healthcare providers who require access to those records. Personal representatives may also act on behalf of patients under certain circumstances. It is essential to have both the patient and facility witness signatures to validate the authorization process fully.
How to Fill Out the Authorization for Use and Disclosure of Protected Health Information Online (Step-by-Step)
-
Begin by entering the patient's name in the designated field.
-
Next, input the date of birth to verify identity.
-
Select the types of records that will be disclosed, such as medical history or treatment records.
-
Ensure all required fields are filled accurately to avoid delays.
-
Review the information for completeness before submitting.
Field-by-Field Instructions for the Authorization for Use and Disclosure of Protected Health Information
Each field in the authorization form has specific requirements that must be met for accurate completion. For instance, under 'Patient Name,' ensure the full legal name is provided. When filling in 'Date of Birth,' the format must follow MM/DD/YYYY for consistency. Address potential confusion about sections with clear examples of how to fill them out correctly.
How to Sign the Authorization for Use and Disclosure of Protected Health Information
Signing the authorization form can be accomplished through either digital or wet signatures, depending on preferences and circumstances. It is important to note witness requirements; both patient and facility representatives must sign to validate the form. For ease of use, pdfFiller offers functionalities for eSigning the document securely.
Submission Methods for the Authorization for Use and Disclosure of Protected Health Information
Completed forms can be submitted via various methods, including in-person delivery to healthcare facilities or through secure online portals depending on establishment guidelines. In New York, different healthcare facilities may have slight variations in their submission processes, so checking individual requirements is recommended. Factors such as processing time and confirmation of receipt should also be considered.
Common Errors and How to Avoid Them When Filing the Authorization for Use and Disclosure of Protected Health Information
When completing the authorization form, users frequently make mistakes such as omitting required signatures or failing to fill out all fields. To avoid these errors, take the time to review each section thoroughly before submission. Accuracy in the details provided is crucial to prevent delays in processing the patient's health information.
Security and Compliance in Handling the Authorization for Use and Disclosure of Protected Health Information
Compliance with GDPR and HIPAA standards is essential for the proper handling of sensitive health information contained in this authorization form. Emphasizing security, pdfFiller ensures that user data is protected with 256-bit encryption and meets rigorous security protocols, making it a reliable option for handling health documents securely.
Empower Your Healthcare Journey with pdfFiller
Utilizing pdfFiller for managing your authorization forms can streamline the process, allowing for easy completion and efficient document management. The platform offers user-friendly features such as eSigning and secure sharing, all while ensuring a commitment to privacy and data security in handling healthcare documentation.
How to fill out the ECMC LGL 100
-
1.Access and open the Authorization for Use and Disclosure of Protected Health Information form on pdfFiller's website by using the provided link or searching for the form title.
-
2.Once open, review the entire document to familiarize yourself with the required information and fields before starting to fill it out.
-
3.Begin filling in your personal information, including your name and date of birth, as indicated by the blank fields provided.
-
4.Select the types of health records to be disclosed by using checkboxes or text fields according to your specific needs.
-
5.Use the information section to clearly state the expiration date of the authorization, ensuring it complies with the relevant privacy laws.
-
6.Provide details about the individuals or entities authorized to receive your health information; type in their names and contact information as necessary.
-
7.Review the completed form for accuracy, ensuring all required fields are filled, and that your intentions for disclosure are clearly stated.
-
8.Once verified, use the signature field to sign the form either by typing your name or using the electronic signature feature.
-
9.Optionally, have a facility witness sign the form in their designated area to fulfill the requirements outlined in the form's instructions.
-
10.After signing, save the completed form to your pdfFiller account. You can also choose to download it in your preferred format or submit it electronically based on any specific submission instructions provided.
-
11.Ensure you have any necessary copies for your records and review any submission deadlines if applicable.

Who can use the Authorization for Use and Disclosure of Protected Health Information?
Patients, personal representatives, and healthcare providers can utilize this form to authorize the release of health information as required by federal privacy regulations.
Is there a time limit on the authorization provided through this form?
Yes, users must specify an expiration date on the form. Without an expiration date, the authorization may remain valid until it is revoked or until the purpose of the disclosure is fulfilled.
What should I do after completing the form?
After completion, ensure to sign the form and have it witnessed, if required. Save the completed document, and review submission methods whether electronic or via postal service.
What supporting documents are required with this authorization form?
Typically, no additional documents are required unless specified by the healthcare provider or institution. However, it may be beneficial to have any identification or previous medical records handy.
What are common mistakes to avoid when filling out this form?
Common mistakes include forgetting to sign the form, omitting required fields, or failing to specify the expiration date. Ensure all information is complete before submission.
How long does it take for the authorization to process?
Processing times can vary based on the receiving facility's policies. Generally, it is advisable to allow several business days for processing after submission.
Can I revoke the authorization after submitting this form?
Yes, individuals can revoke the authorization at any time by notifying the healthcare provider or entity that received the original authorization, but they may need to follow specific procedures to do so.
ECMC LGL 100 Form Versions
Related Content
Related Forms



Related Catalogs

If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.