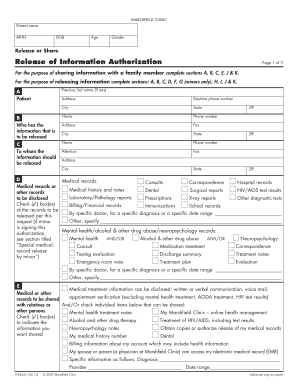
What is medical record authorization for release of information?
Medical record authorization for release of information is a legal document that gives consent to healthcare providers to disclose an individual's medical records to a third party. It is necessary for the smooth sharing of medical information between healthcare providers, insurance companies, attorneys, and other authorized entities. This authorization ensures the privacy and confidentiality of the patient's medical records while allowing the necessary information to be shared for treatment, insurance claims, legal proceedings, and other purposes.
What are the types of medical record authorization for release of information?
There are different types of medical record authorization forms depending on the specific purpose. Some common types include:
General Authorization: This type of authorization allows the release of all medical records for any purpose specified by the patient.
Limited Authorization: It restricts the release of medical records to specific healthcare providers or for a particular purpose.
Consent for Minors: This form is used when a minor's medical records need to be accessed by parents or legal guardians.
Consent for Mental Health Records: This form is required when mental health records are being disclosed.
Consent for Sensitive Information: Certain sensitive medical information, such as HIV status or substance abuse treatment, requires specific consent for disclosure.
How to complete medical record authorization for release of information
Completing a medical record authorization for release of information form is a simple process. Here are the steps to follow:
01
Identify the purpose: Determine why you need to release your medical records and select the appropriate authorization form.
02
Provide personal information: Fill in your full name, date of birth, contact information, and any other required identification details.
03
Specify the recipient: Indicate the healthcare provider, insurance company, attorney, or any other authorized entity to whom you are authorizing the release of your medical records.
04
Sign and date the form: Review the completed form, sign it, and include the date of authorization.
05
Submit the form: Send the completed form to the designated recipient through secure means such as mail, fax, or electronic submission.
pdfFiller empowers users to create, edit, and share documents online. Offering unlimited fillable templates and powerful editing tools, pdfFiller is the only PDF editor users need to get their documents done.