Countersign Professional Medical History For Free


Users trust to manage documents on pdfFiller platform
Send documents for eSignature with signNow
Watch a quick video tutorial on how to Countersign Professional Medical History
pdfFiller scores top ratings in multiple categories on G2
Countersign Professional Medical History with the swift ease
pdfFiller enables you to Countersign Professional Medical History quickly. The editor's convenient drag and drop interface allows for quick and intuitive signing on any operaring system.
Ceritfying PDFs electronically is a fast and safe way to verify papers anytime and anywhere, even while on the fly.
Go through the step-by-step instructions on how to Countersign Professional Medical History online with pdfFiller:
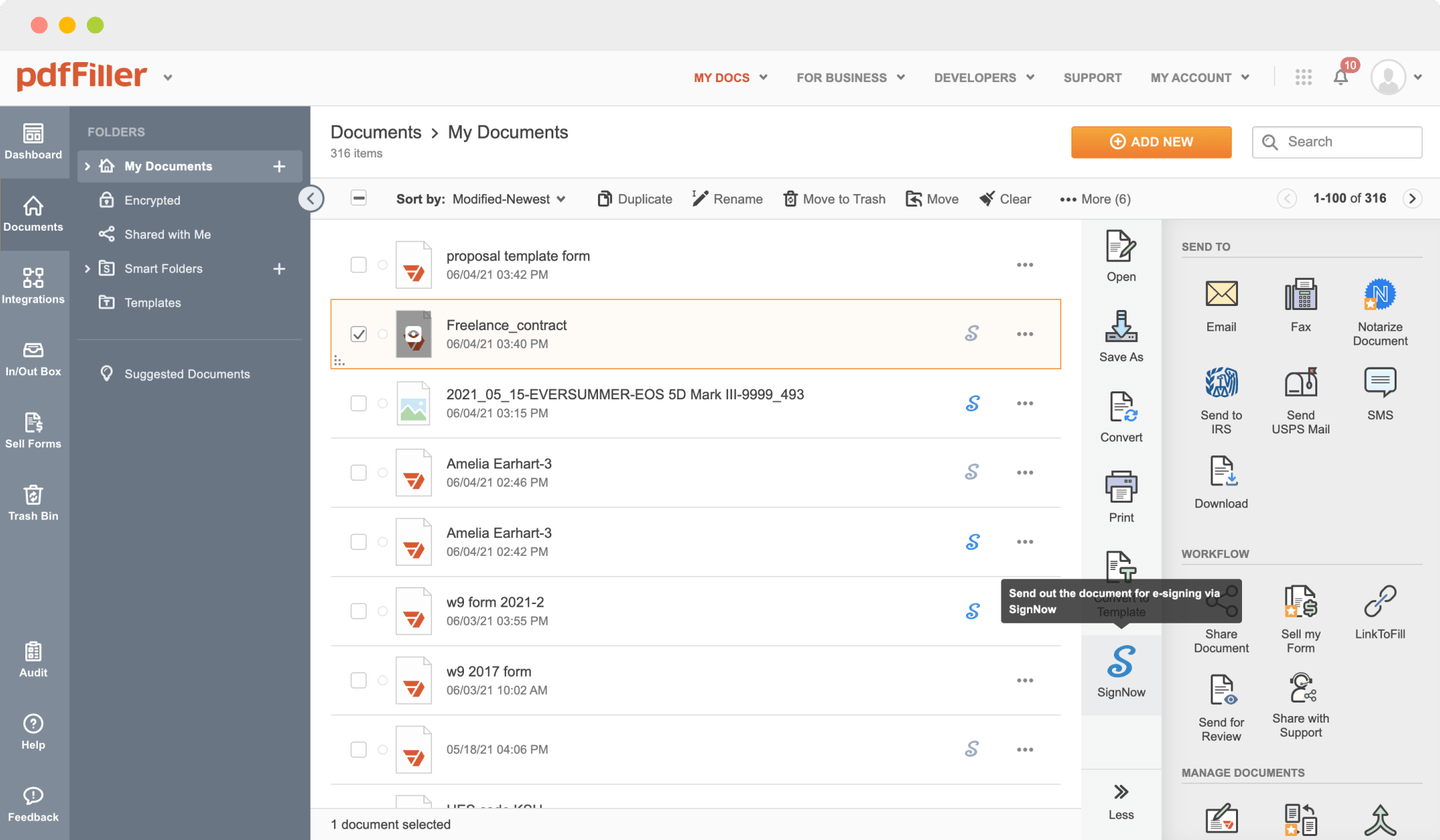
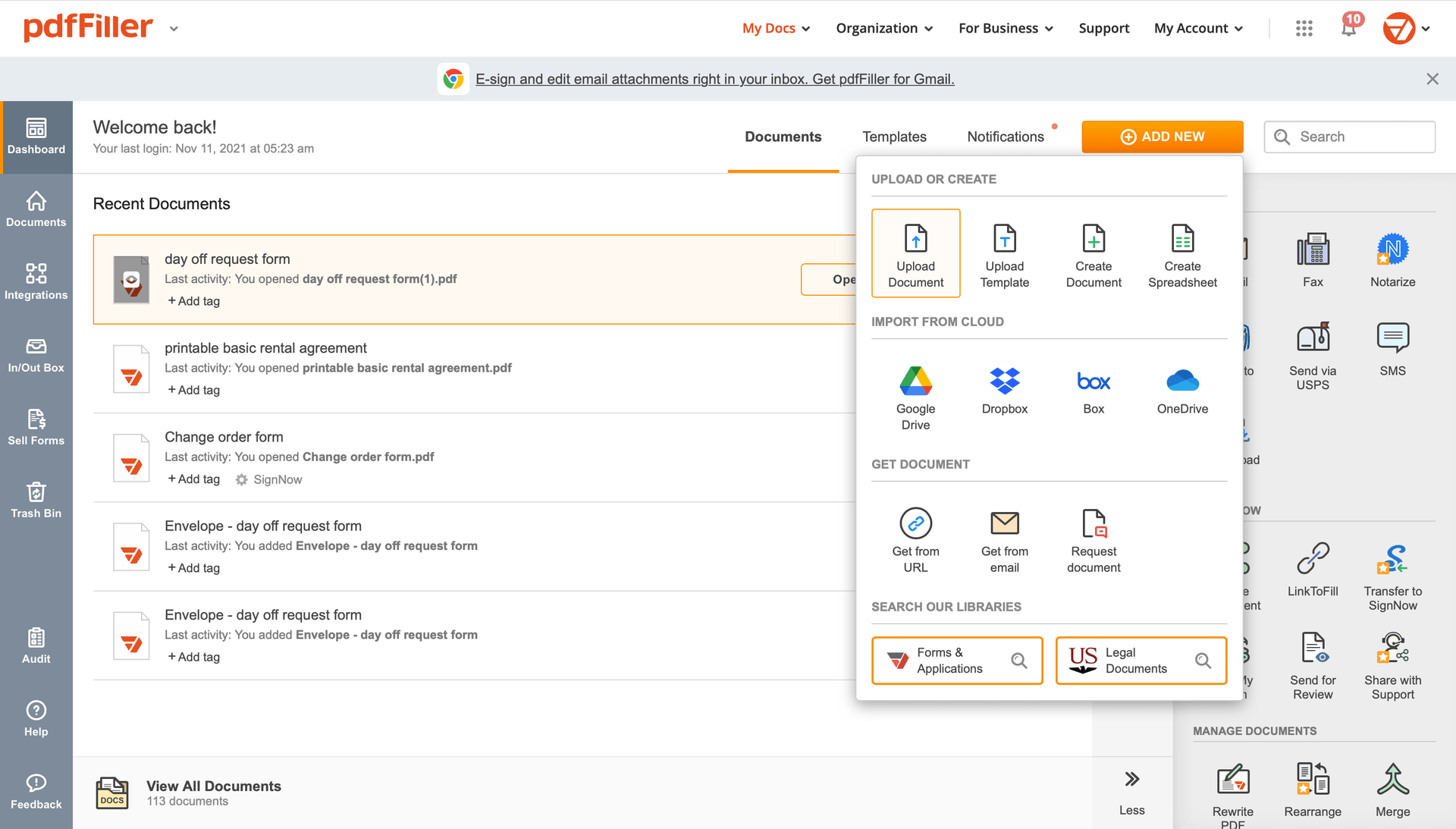
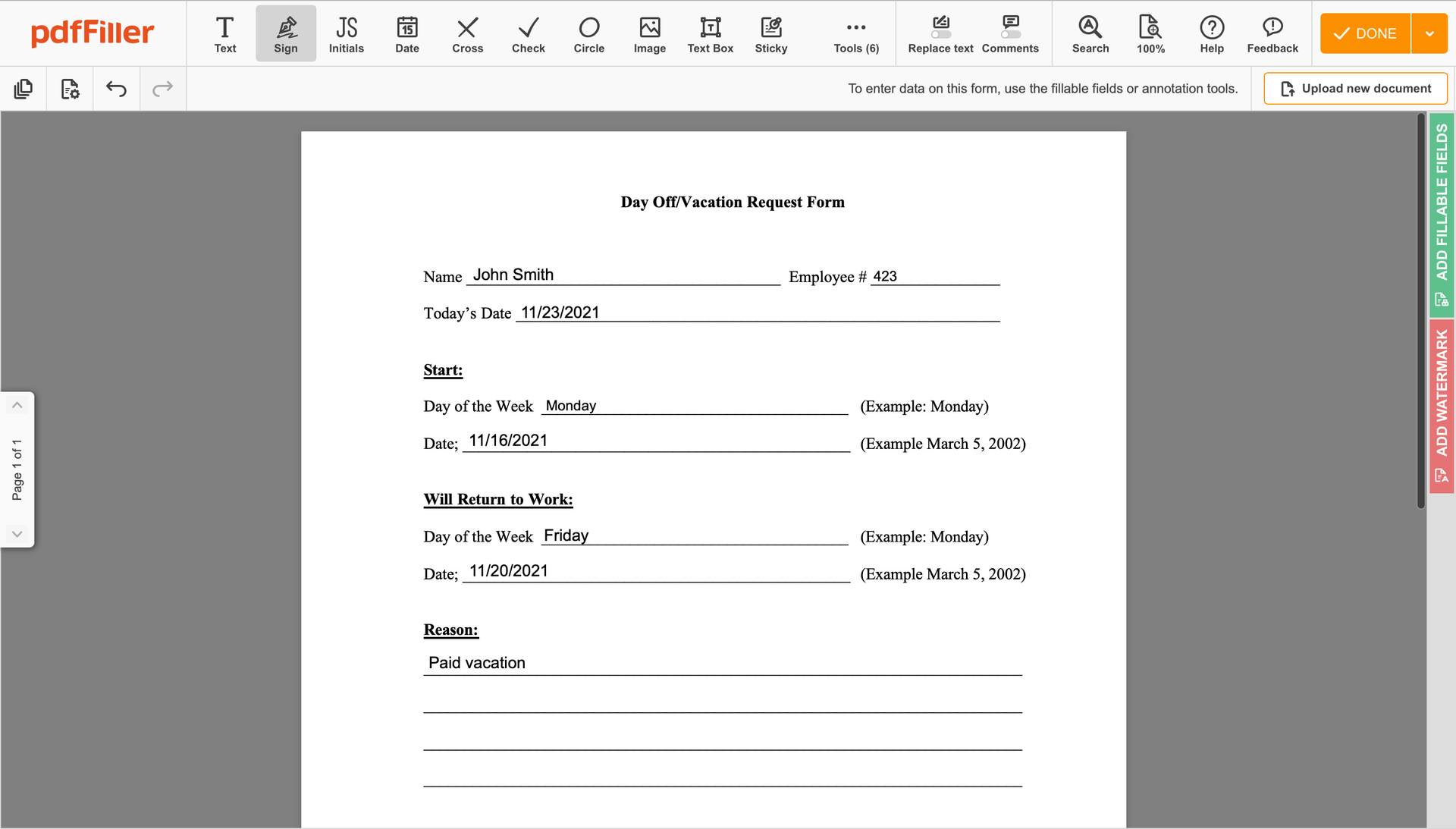
Upload the document you need to sign to pdfFiller from your device or cloud storage.
As soon as the file opens in the editor, hit Sign in the top toolbar.
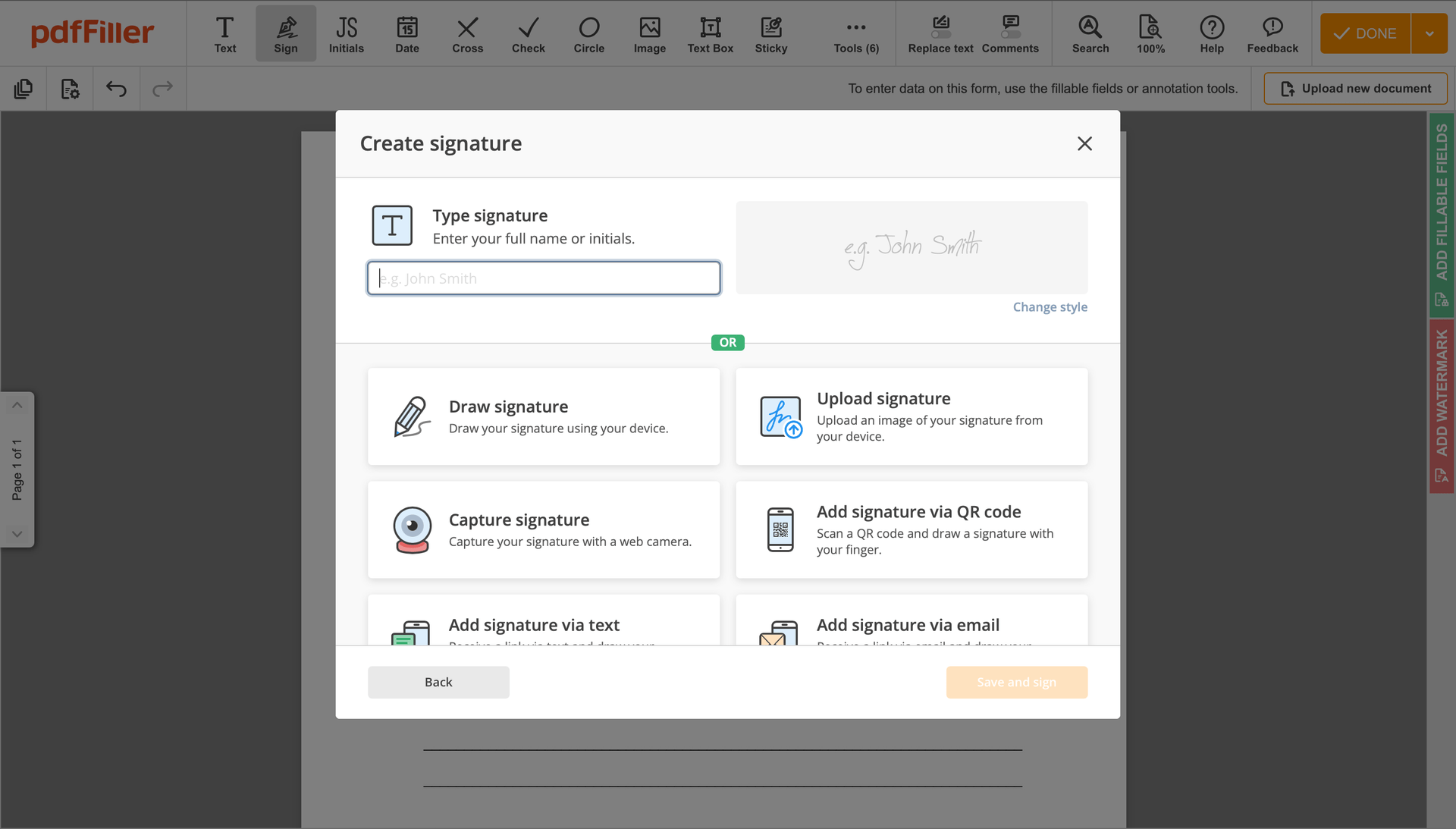
Generate your electronic signature by typing, drawing, or uploading your handwritten signature's image from your laptop. Then, hit Save and sign.
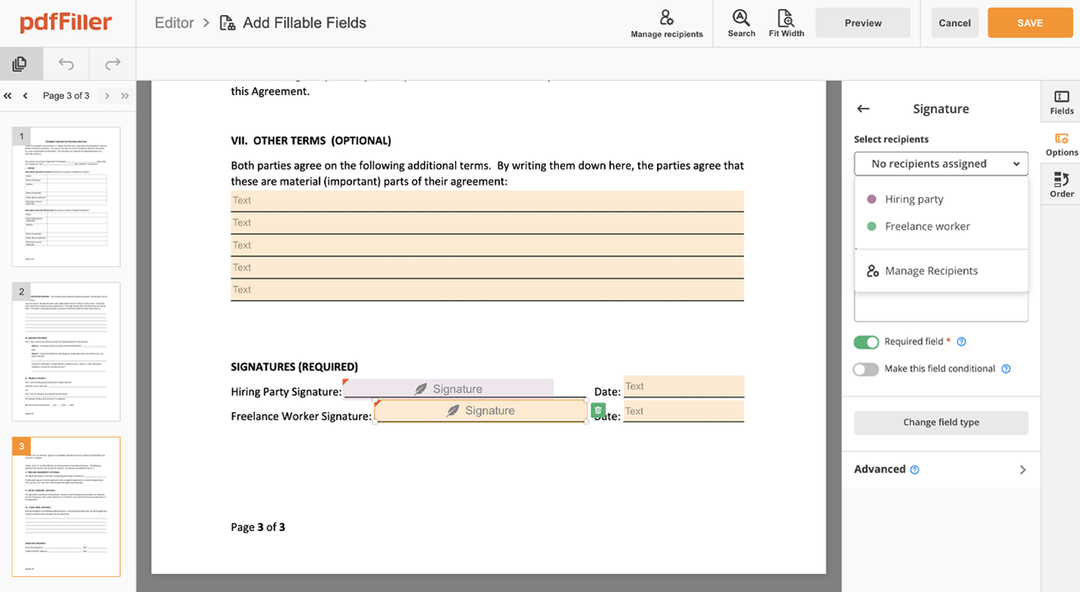
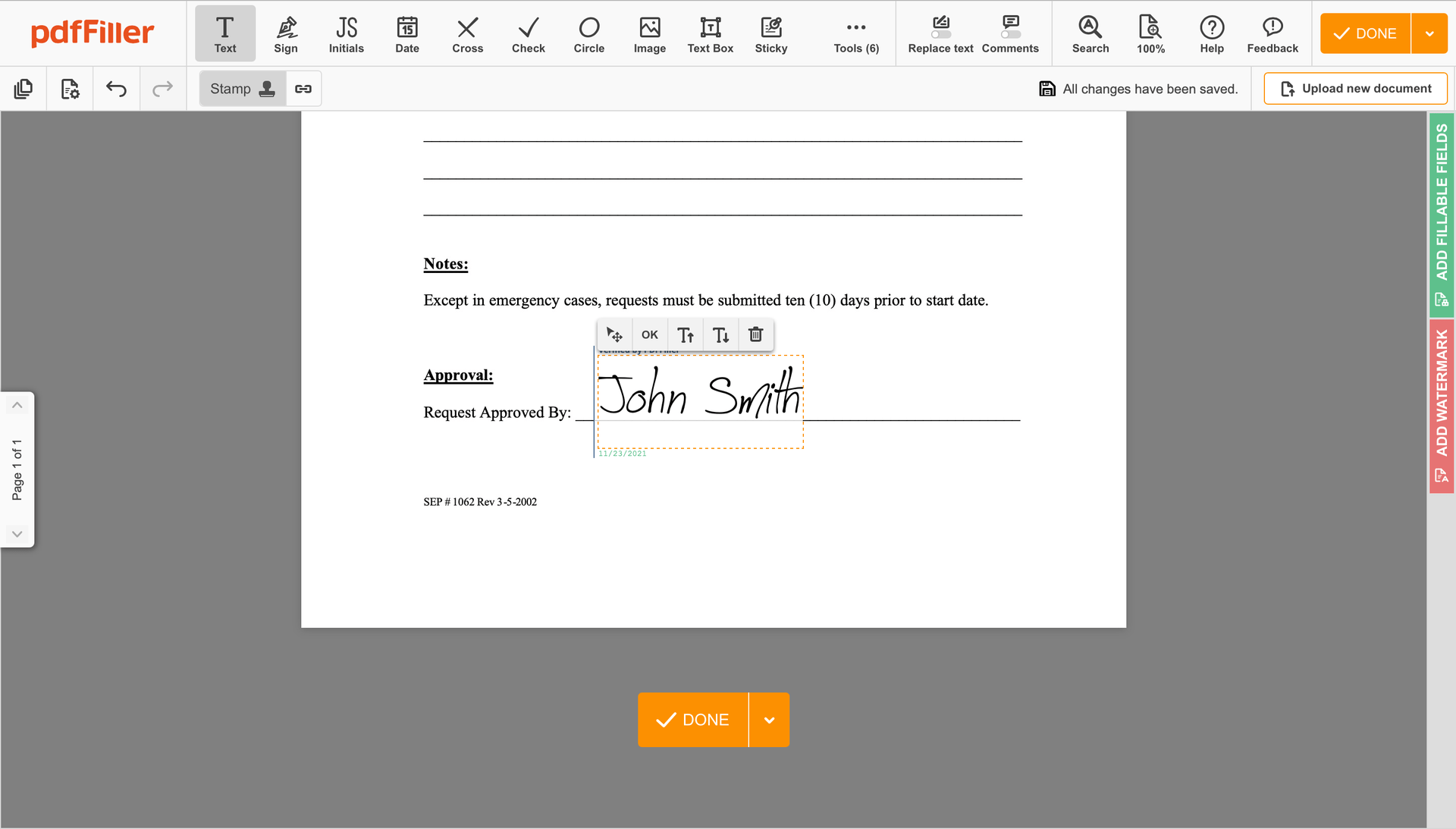
Click anywhere on a form to Countersign Professional Medical History. You can move it around or resize it utilizing the controls in the floating panel. To use your signature, hit OK.
Complete the signing session by clicking DONE below your form or in the top right corner.
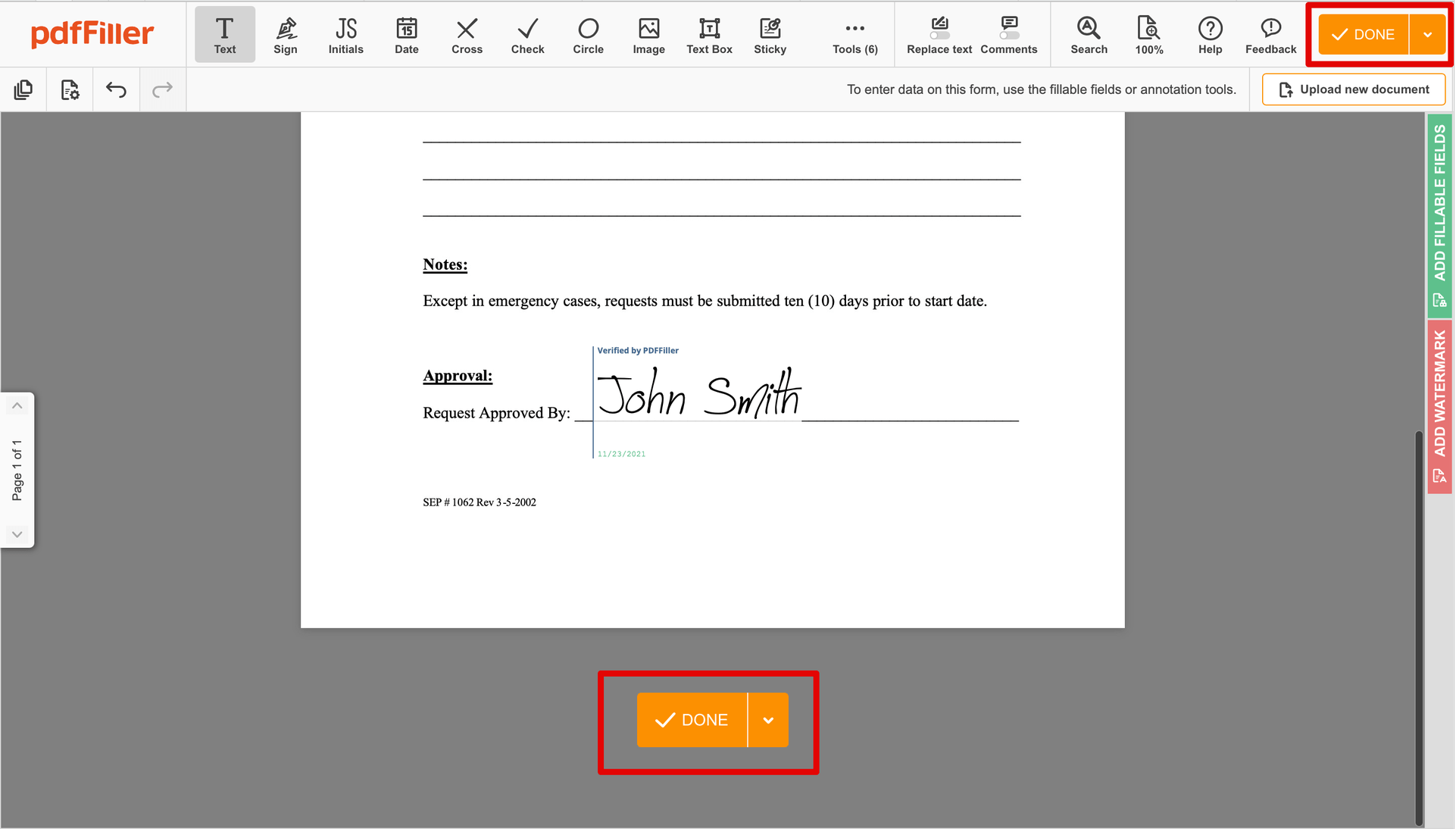
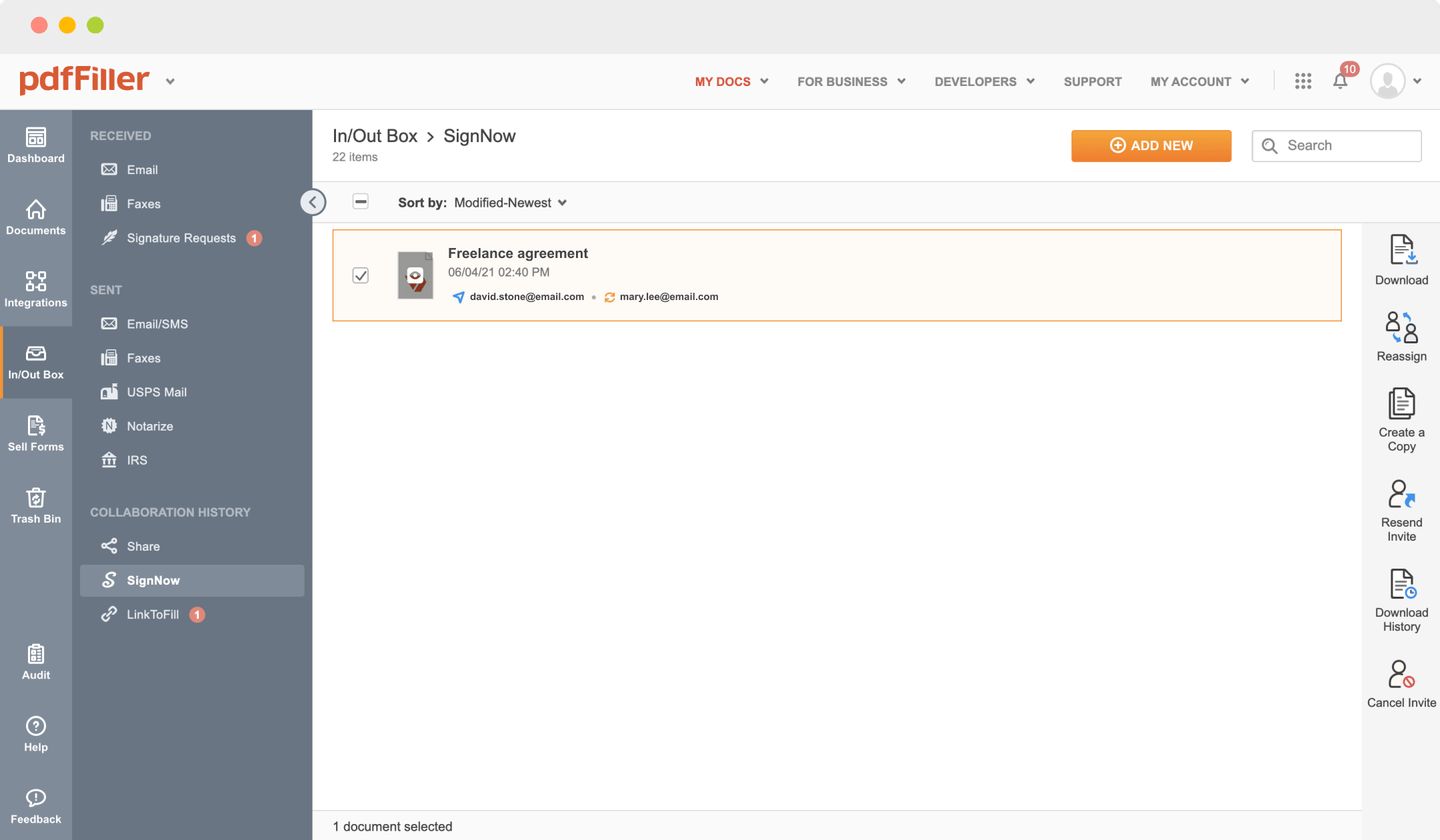
After that, you'll go back to the pdfFiller dashboard. From there, you can download a completed copy, print the form, or send it to other parties for review or approval.
Stuck working with numerous applications for managing documents? We've got a solution for you. Use our document management tool for the fast and efficient process. Create fillable forms, contracts, make templates, integrate cloud services and utilize more useful features within your browser. Plus, you can use Countersign Professional Medical History and add unique features like signing orders, alerts, requests, easier than ever. Get a significant advantage over those using any other free or paid tools.
How to edit a PDF document using the pdfFiller editor:
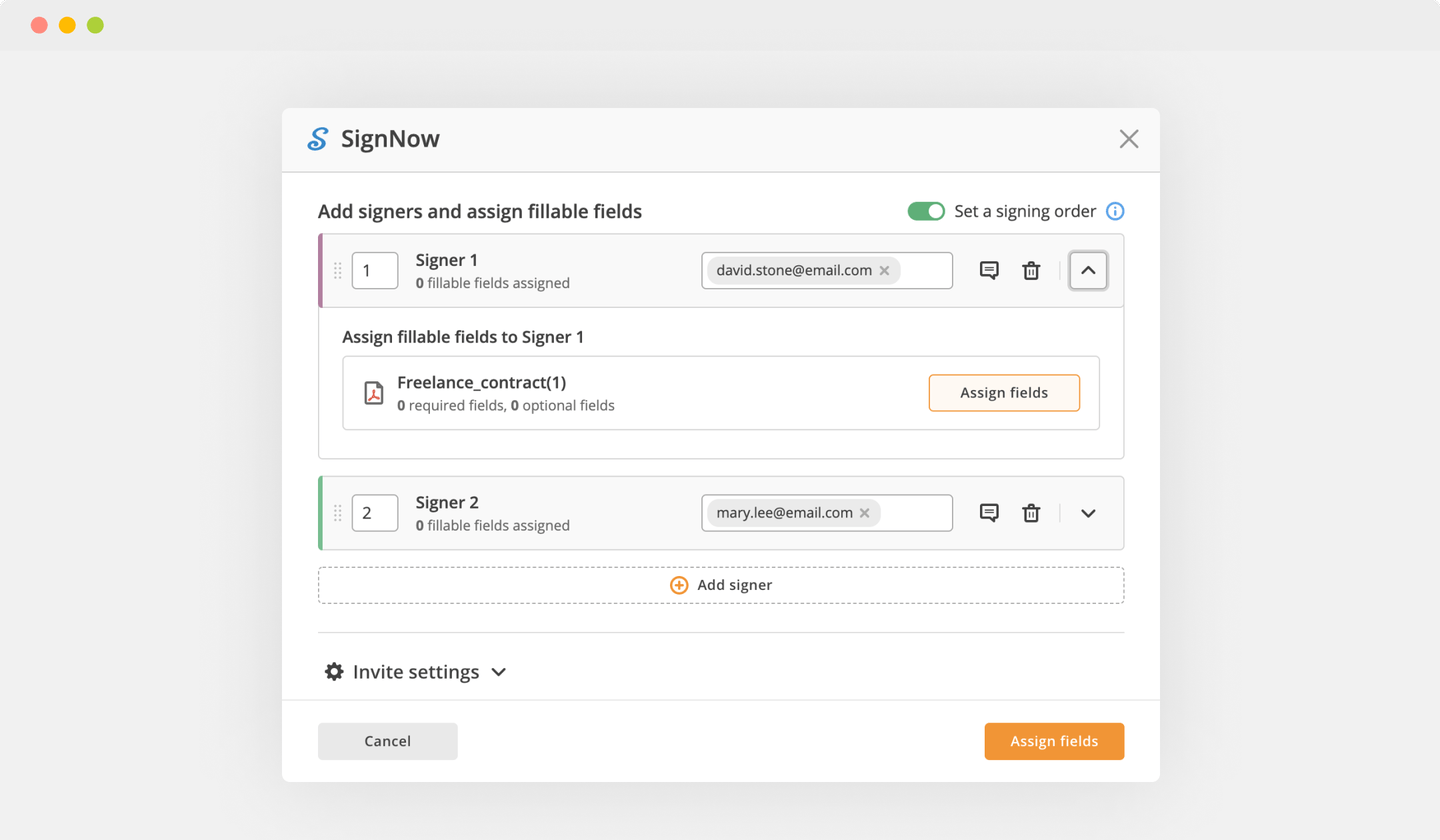
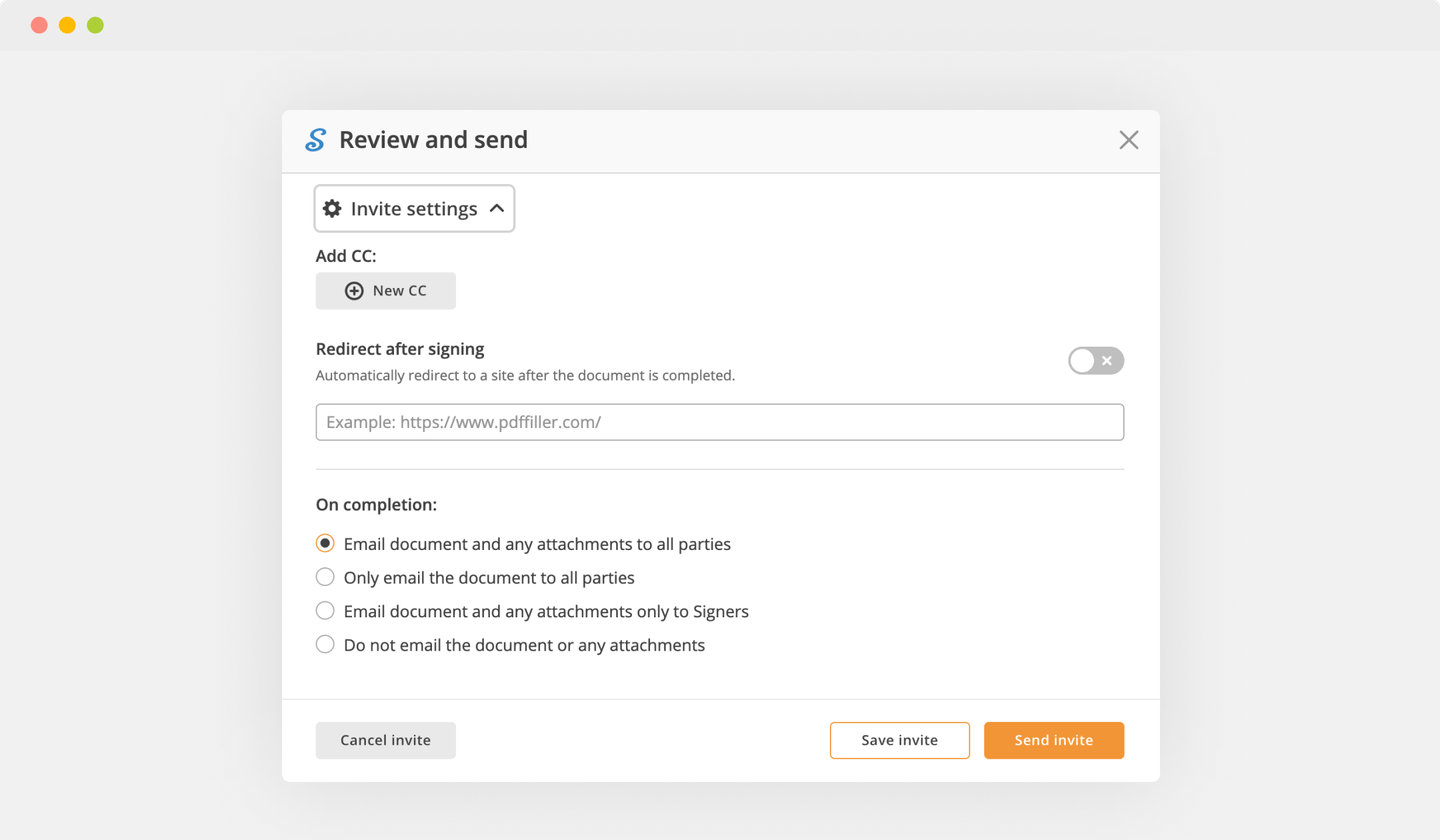
How to Send a PDF for eSignature
Related features
What our customers say about pdfFiller
That I am able to take any non-fillable pdf document and make it fillable.
What do you dislike?
I find the ease of use of the website decreased with the updated version. Not impossible, but less ease of use. Nothing too bad.
What problems are you solving with the product? What benefits have you realized?
I use pdfiller in all aspects of my job where non-fillable documents are not available. From Business Management to Human Resources.


